Two Failing Organs and a Rare Comorbidity
In early 2021, a 55-year-old man with a history of polycystic kidney disease and end-stage renal disease presented to an emergency room in New Jersey with cardiogenic shock. After progressing to refractory cardiogenic shock, he was transferred to NYU Langone from Morristown Medical Center, part of the Atlantic Health System, a new affiliate of NYU Langone’s Transplant Institute, where he was found to have evidence of an infiltrative cardiomyopathy.
As the man’s condition continued to deteriorate, it became evident that his only hope of survival lay in a dual heart and kidney transplant. Judging that he was too ill to endure such an operation, however, surgeons at NYU Langone’s Transplant Institute turned to a stopgap measure that only a handful of centers worldwide have the resources to apply: an artifical heart.
“Very few transplant programs would have taken on a case like this… Our collective skills and experience, as well as our robust clinical infrastructure, gave us the confidence to say yes.”
Nader Moazami, MD
Within a week, the Transplant Institute secured a SynCardia 70cc Total Artificial Heart (TAH) and trained a team of 143 clinical specialists on the highly complex device. The six-hour surgery was led by Nader Moazami, MD, chief of the Division of Heart and Lung Transplant and Mechanical Circulatory Support.
Pathology on the patient’s explanted heart demonstrated amyloid light-chain (AL) amyloidosis. Members of NYU Langone’s Amyloidosis Center collaborated closely with the heart and kidney transplant programs to create a strategic plan incorporating subsequent treatment for his infiltrative condition alongside immunosuppression.
In June, after undergoing intensive rehabilitation, the patient underwent a heart-kidney transplantation, and was discharged home 15 days later. While continuing to receive outpatient chemotherapy, he has had no significant rejection, and has resumed a normal life.
“Very few transplant programs would have taken on a case like this because of the complexities involved at every stage of treatment,” Dr. Moazami observes. “Our collective skills and experience, as well as our robust clinical infrastructure, gave us the confidence to say yes.”
A Grim Prognosis

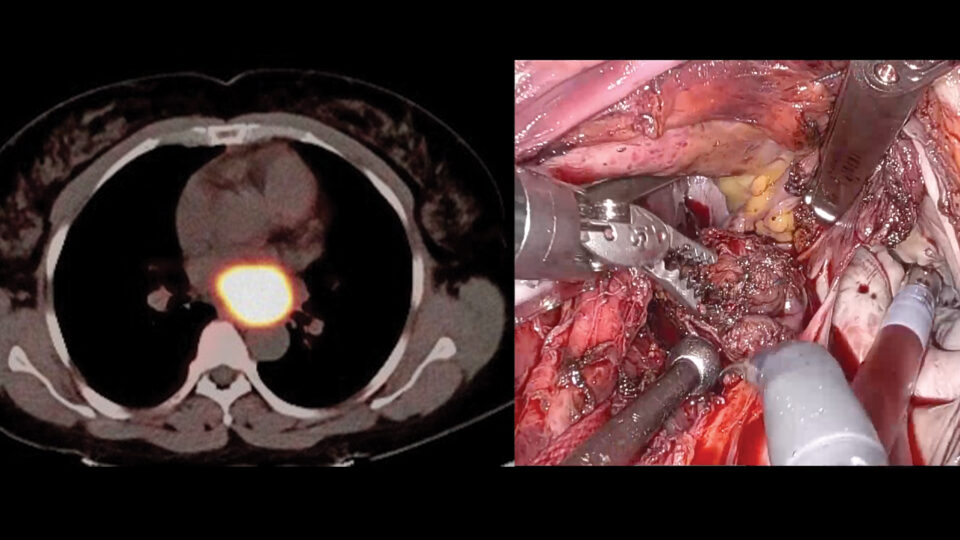
The patient’s echocardiogram on admission.
On admission, the patient’s echocardiogram showed substantial cardiomyopathy. “His heart was big and thick, he had markers of kidney and liver failure, including dramatically elevated lactate and bilirubin levels,” says Alex Reyentovich, MD, director of the Heart Failure Program.
Amyloidosis Complicates the Picture
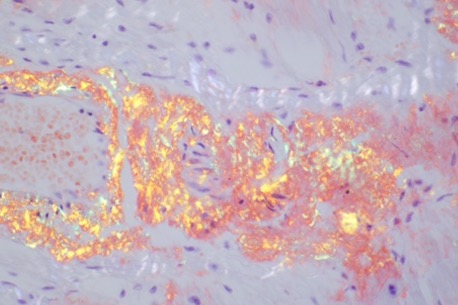
A Congo Red-stained slide of the patient’s heart tissue.
Cardiac biopsy revealed undiagnosed AL amyloidosis as the underlying cause of the patient’s heart failure. Developing a long-term treatment plan in the context of immunosuppression required careful coordination between multidisciplinary transplant, amyloidosis, and hematology teams.
Stabilizing the Patient: Implantation and Rehabilitation
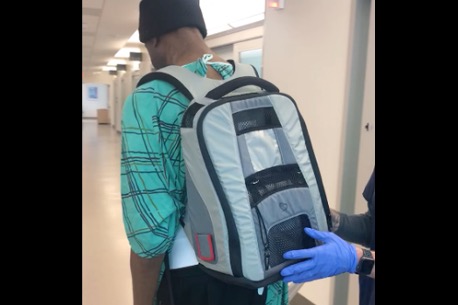
After implantation of the artificial heart, the patient carries the portable system on a walk with physical therapists.
The patient had to be stabilized before he could undergo dual transplant surgery. First, he was implanted with a SynCardia Total Artificial Heart (TAH) in a six-hour surgery led by Dr. Moazami. Then, he began a course of rehabilitation designed to strengthen him further. Within a month, he was able to carry the TAH’s pneumatic driver in a backpack.
From TAH to Dual Transplant

Dr. Nader Moazami and team performing surgery.
Five weeks after receiving the TAH, the patient underwent heart-kidney transplantation. NYU Langone performs over 10 such dual transplants per year, with a 100 percent one-year survival rate (compared to 88.5 percent nationwide).