In November 2025, a man in his early 60s with symptomatic obstructive hypertrophic cardiomyopathy (HCM) was referred to cardiologist Daniele Massera, MD, associate director of NYU Langone Health’s Hypertrophic Cardiomyopathy Program, for evaluation. The patient had been treated with mavacamten by a cardiologist at an outside institution but had an incomplete response. Additionally, he had grown tired of the time-consuming logistics associated with lifelong cardiac myosin inhibitor therapy. He wanted a “one and done” surgical solution in lieu of the frequent appointments and echocardiogram monitoring required for medical management.
“We initially discussed an open septal myectomy through a median sternotomy,” Dr. Massera says. But the patient wasn’t satisfied. When he asked about a minimally invasive surgical alternative, Dr. Massera referred him to robotic cardiac surgeon, and associate surgical director of the HCM program, Joshua A. Scheinerman, MD.
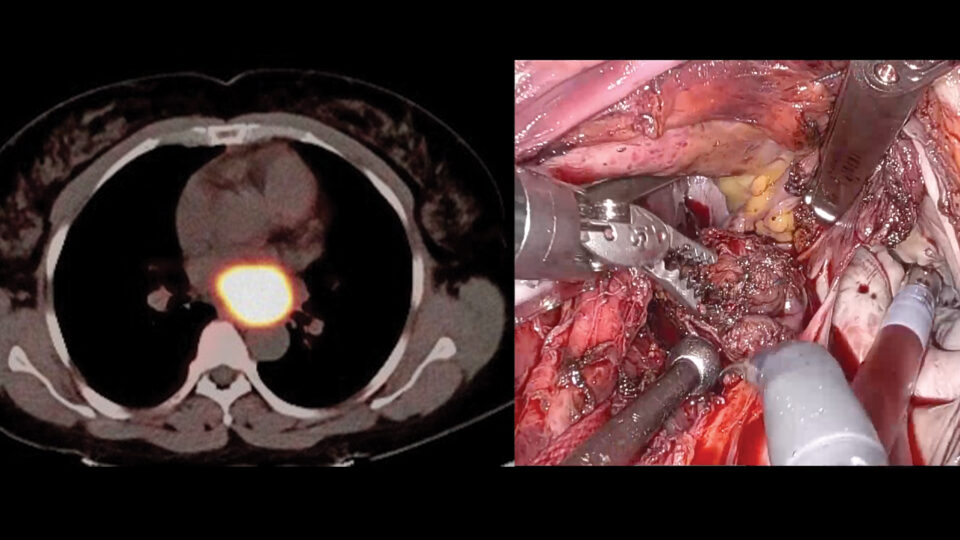
Given the patient’s significantly elevated left ventricular outflow tract (LVOT) gradient, along with his life-limiting symptoms and desire for a durable solution, he was an ideal candidate for surgical myectomy. In light of Dr. Scheinerman’s extensive experience with robotic cardiac operations, a robotic approach was offered for this curative procedure. It would represent the first robotic septal myectomy for obstructive HCM performed at NYU Langone.
“We are one of the only high-volume, dedicated HCM programs in the United States to offer robotic septal myectomy for select patients with obstructive HCM.”
Joshua A. Scheinerman, MD
“We are the one of the only high-volume, dedicated HCM programs in the United States—and the only one in New York—to offer robotic septal myectomy for select patients with obstructive HCM,” Dr. Scheinerman says.
Surgical Approach
The four-hour operation was led by Dr. Scheinerman, Eugene A. Grossi, MD, the Stephen B. Colvin, MD, Professor of Cardiothoracic Surgery and director of cardiac surgical research, and cardiac anesthesiologist Robert G. Nampi, MD.
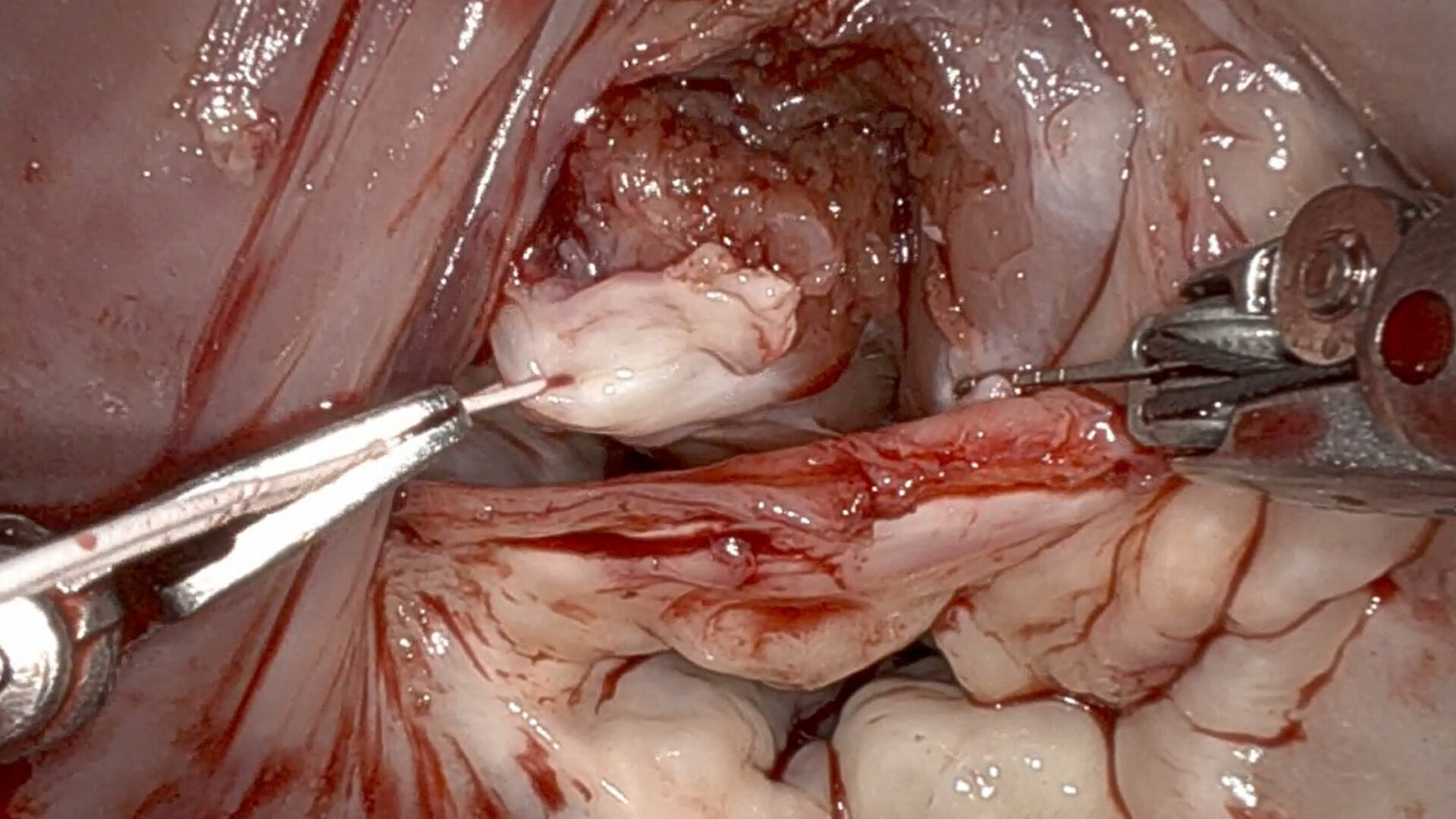
Four ports were placed in the right chest to facilitate a totally endoscopic robotic approach. Dr. Scheinerman opened the left atrium, exposing the mitral valve and left atrial appendage. The left atrial appendage was closed to prevent future stroke, and a modified cryoablation maze procedure was performed to treat the patient’s yearslong burden of atrial fibrillation.
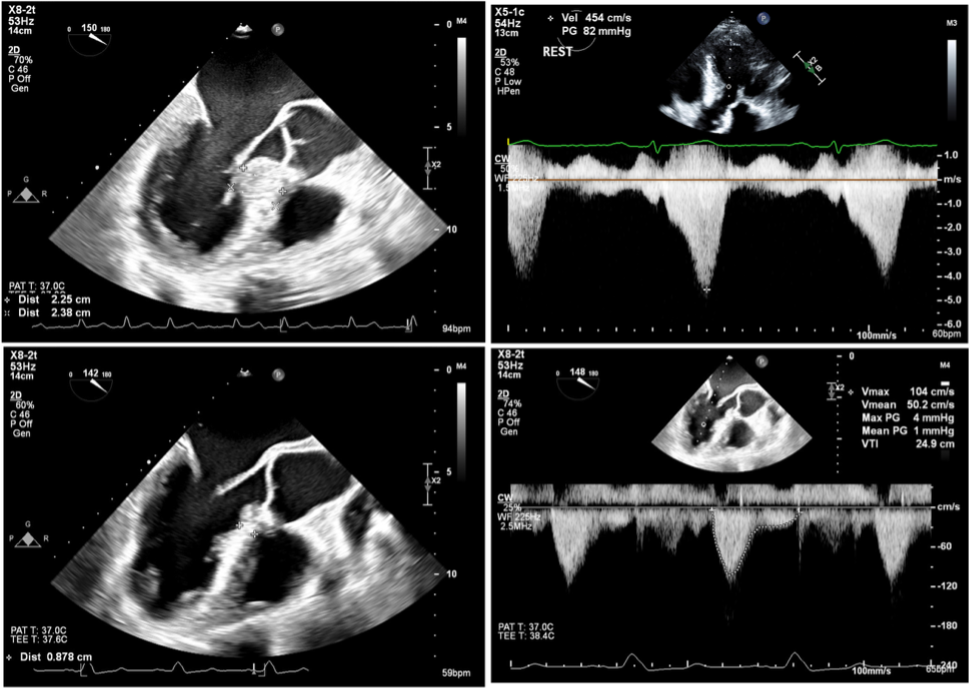
Turning to the mitral valve, an incision was made in the anterior leaflet to expose the interventricular septum. Using robotic instrumentation, Dr. Scheinerman performed the septal myectomy from the basal to apical septum. The extent of resection was guided by preoperative transthoracic and transesophageal echocardiography as well as structural CT imaging. Approximately 10 mm in depth and 40 mm in length of septal myocardium was resected to achieve adequate relief of LVOT obstruction.
After reconstructing and inspecting the mitral valve, hydrostatic saline testing confirmed the absence of significant regurgitation. The left atrium was closed and the heart resumed spontaneous sinus rhythm. The patient was extubated in the operating room and transferred to the cardiac ICU in stable condition.
Postoperative Outcome
Postoperative transesophageal echocardiography demonstrated a superb result: significantly reduced septal thickness, absence of systolic anterior motion of the mitral valve, elimination of LVOT obstruction, trace mitral regurgitation, and no ventricular septal defect. The patient was discharged on postoperative day four.
“A robotic approach through the left atrium opens up new and exciting avenues to address outflow tract obstruction,” Dr. Scheinerman says. “In many ways, exposure through a window created in the mitral valve creates even better access, feasibility of septal muscle resection, and LVOT augmentation compared to the traditional open approach. Most importantly,” he adds, “this will result in elimination of outflow tract gradient and provide complete symptomatic relief to patients, all while sparing them a large midline incision.”
“The patient couldn’t be happier that he underwent successful septal myectomy surgery without requiring a median sternotomy and will no longer require medical therapy for obstructive HCM.”
Daniele Massera, MD
While the patient’s outflow tract obstruction was successfully relieved and his atrial fibrillation was treated with intraoperative cryoablation, there is still a small risk of future episodes of atrial fibrillation. Given this, he will require anticoagulant medication.
Overall, the patient is thrilled with his outcome. “The patient couldn’t be happier that he underwent successful septal myectomy surgery without requiring a median sternotomy, no longer requires medical therapy for obstructive HCM, and will only need to return once a year for follow-up,” Dr. Massera says.
“Many patients with symptomatic obstructive HCM will be candidates for this robotic surgical approach,” Dr. Scheinerman adds.