Bladder Preservation Poses a Difficult Dilemma
Having deferred radical cystectomy for years, a patient with a long history of recurrent high-risk non-muscle-invasive bladder cancer (NMIBC), who became unresponsive to bacillus Calmette-Guérin (BCG), responded well after ultimately undergoing surgery and urinary diversion.
According to Gary D. Steinberg, MD, director of the Goldstein Urology Bladder Cancer Program at Perlmutter Cancer Center, the case is representative of a common clinical conundrum—is it safe to defer or avoid radical cystectomy for BCG-unresponsive high-risk disease?
While radical cystectomy is highly curative, many patients decline to undergo the procedure due to the life-altering consequences and reduced quality of life.
“The risk of progression to muscle invasion and/or metastatic disease is greatly increased for patients with high-grade non-muscle invasive bladder cancer that does not respond to BCG,” Dr. Steinberg says. “In general, progression may occur within six to 12 months.”
The patient, a white male in his 70s, was initally diagnosed in 2011 with T1 high-grade NMIBC. In addition to BCG, his prior treatment history included mitomycin-C and interferon (IFN)-α.
“The patient reports improved quality of life with his ileal conduit urinary diversion which has eliminated his irritative voiding symptoms and incontinence episodes.”
Gary D. Steinberg, MD
After presenting to NYU Langone Health in 2019 for evaluation and management, the patient was diagnosed with BCG-unresponsive carcinoma in situ of the bladder and counselled on radical cystectomy—being the standard of care per national and international guidelines—as well as alternative therapies and clinical trials.
Aiming to preserve his bladder, the patient opted to enroll in CheckMate 9UT*. He was assigned to the three-drug arm and began treatment. When pathology revealed recurrence at six-month follow-up, the patient elected to undergo radical cystectomy and ileal conduit urinary diversion. Due to urothelial carcinoma involving the prostatic urethra, urinary diversion through orthotopic neobladder reconstruction was contraindicated.
The patient regained significant function four weeks after surgery and currently shows no evidence of disease.
“The patient reports improved quality of life with his ileal conduit urinary diversion which has eliminated his irritative voiding symptoms and incontinence episodes,” Dr. Steinberg says.
*The CheckMate 9UT trial closed without reaching accrual goals due to low patient enrollment caused by the BCG shortage and the COVID-19 pandemic.
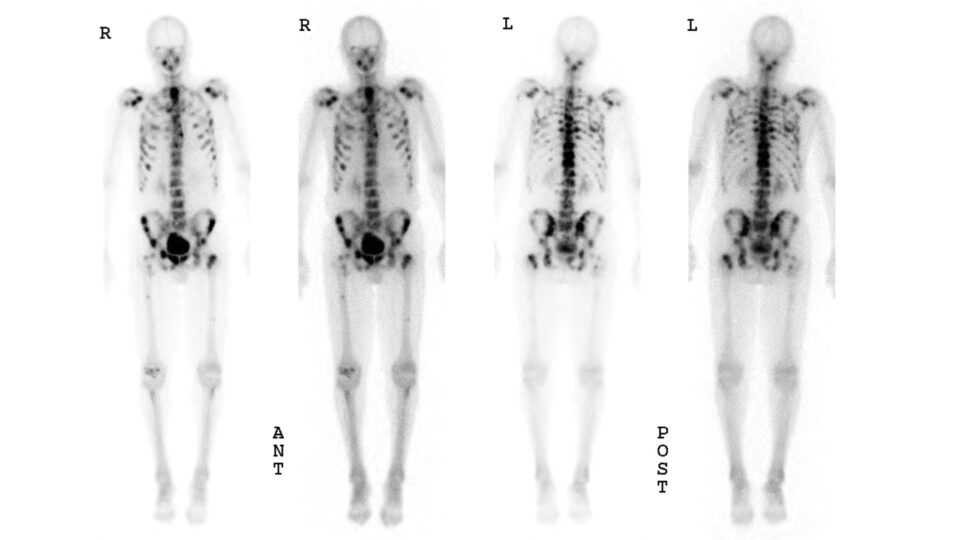
Enrollment in the CheckMate 9UT Trial

Patient’s CT urogram prior to enrollment in CheckMate 9UT. SOURCE: NYU Langone Staff
The patient presented with a history of high-risk NMIBC that persisted and recurred despite intravesical BCG immunotherapy. Choosing to avoid radical cystectomy, the patient elected to enroll in CheckMate 9UT, a phase 2 combination immunotherapy study, and was enrolled to the three-drug arm—nivolumab with linrodostat with BCG.
Cancer Recurrence
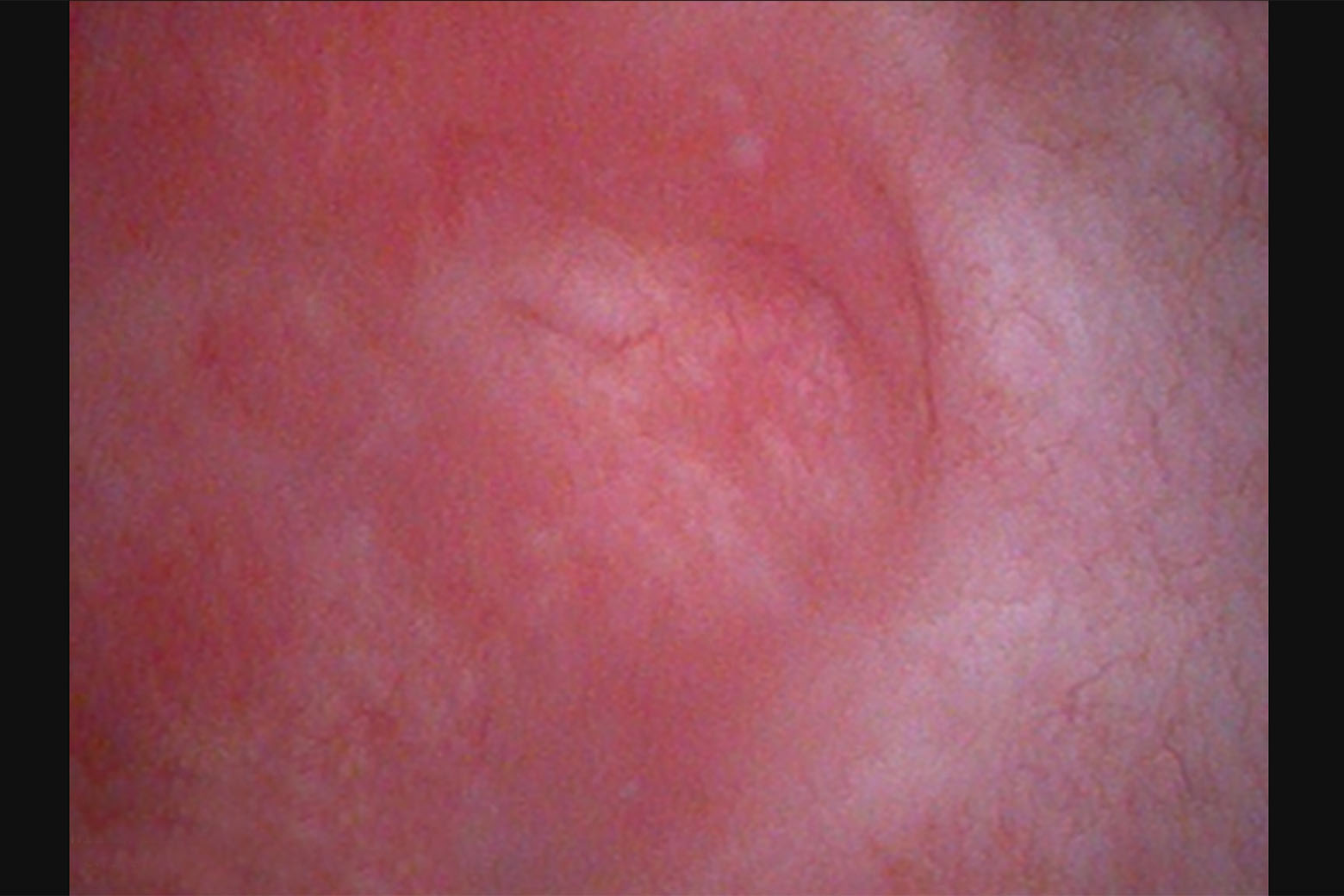
Image from cystoscopy revealing diffuse erythema, inflammation and carcinoma in situ. SOURCE: NYU Langone Staff
After completing treatment, complete response was noted at first response assessment. However, cystoscopy at six-month follow-up revealed a multifocal necrotic tumor as well as multiple papillary/sessile tumors with more than 5 centimeters bladder involvement. Pathology confirmed carcinoma in situ of the right bladder wall, anterior bladder wall, and prostatic urethra.
Observations During Radical Cystectomy
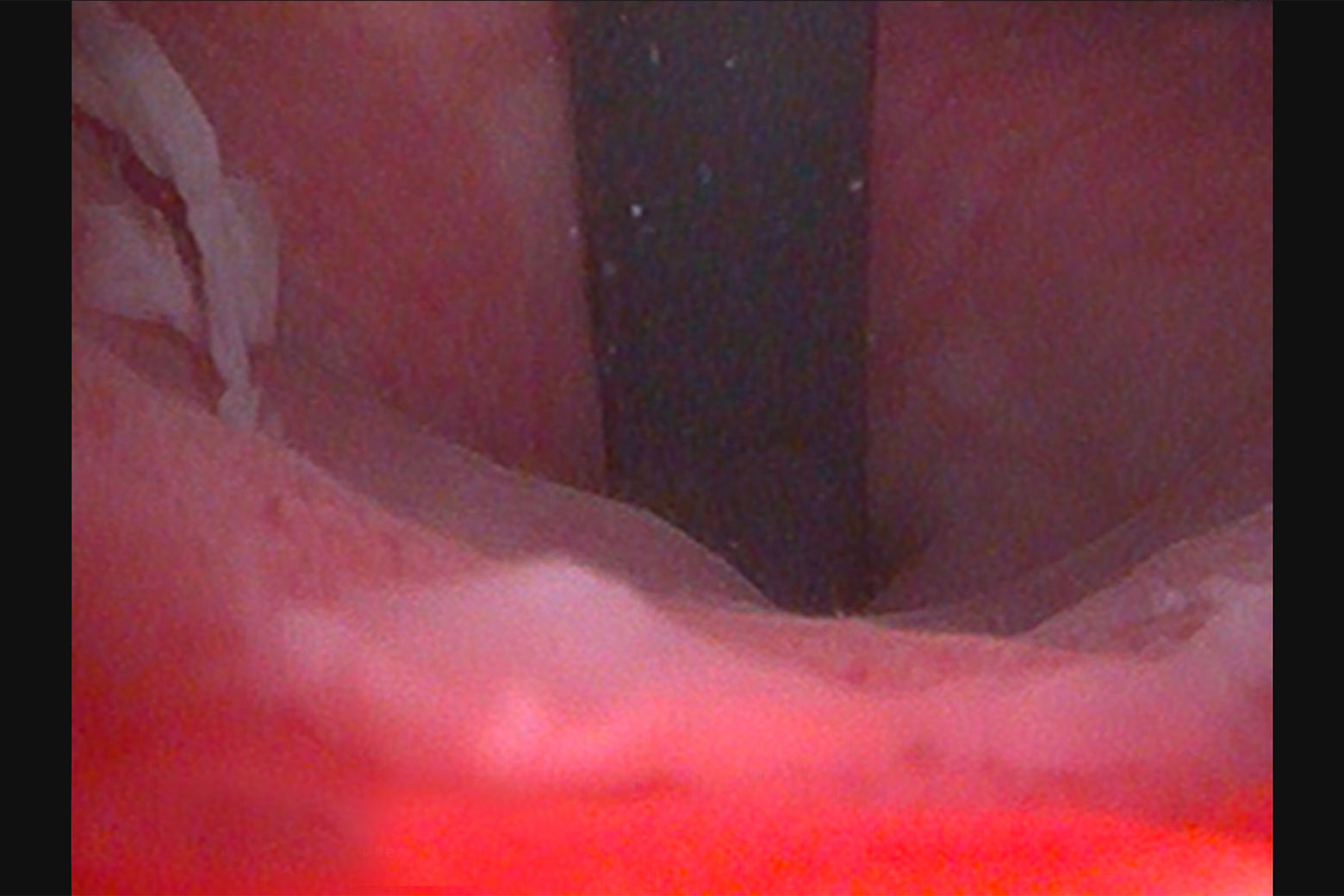
Image from cystoscopy revealing diffuse erythema, inflammation, and carcinoma in situ. SOURCE: NYU Langone Staff
The patient ultimately elected radical cystectomy and urinary diversion. While the surgery was uncomplicated, during the procedure the patient was noted to have bilateral hydroureteronephrosis, dense pelvic lymph nodes with some enlarged lymph nodes, dense scar tissue and fibrosis, and a short, thick wall intestinal mesentery.