More than 1 in 4 adults in the United States have some type of a disability. Although not always readily apparent, these disabilities often interfere with patients’ ability to access quality healthcare.
Megan A. Morris, PhD, one of the foremost experts on healthcare disparities linked to disabilities, joined NYU Langone Health in 2024. Dr. Morris has been at the vanguard of efforts to address the sometimes deadly effects of ableism and to improve both EHR documentation and healthcare services for people with disabilities. Here, she talks about her successes, priorities, and recent initiatives.
Physician Focus: Dr. Morris, one major part of your work is on better documentation of patients’ disability status. Why is that so important?
Dr. Morris: There was a report from The Joint Commission in 2010 that recommended documenting patients’ mobility and communication needs, and then the Department of Justice said health systems need to be documenting patients’ disability status in their medical charts. But no one was talking about it, and no one was doing research. So pretty early on, I started down this path of developing the evidence for what questions we should be asking, how we should be asking the questions, and how we should be training our staff to ask the questions.
“You can’t figure out who needs an accommodation if you’re not first asking who has a disability.”
Megan Morris, PhD
I currently have an R01 grant for a multisite trial on implementing the collection of disability status in the EHR, and then using that information to inform the provision of disability-related accommodations.
There are two purposes for documenting disability status. One is so we can track quality of care at an organization level. If we’re going to develop and implement interventions to address disparities, we need to know who to recruit and how we measure their effects. The second is that health systems are federally required to provide disability accommodations to any patient with a disability who needs it. You can’t figure out who needs an accommodation if you’re not first asking who has a disability.
Physician Focus: How has your work helped change documentation policies?
Dr. Morris: I and a few other researchers worked with the Office of the National Coordinator for Health Information Technology, the federal body that oversees regulations for EHRs, to make disability a required data element for all EHRs.
The largest EHR is Epic, which NYU Langone uses, and they have the disability data elements available on all of their EHRs. They relied heavily on our research to define those disability categories. While that takes care of the back end, where the data lives, you still have to build out the front end so clinicians can enter the data and have it display on a patient’s chart. Our current grant is for creating that build-out.
The ultimate goal is that this feature, which will be included in Epic Foundation, will be a required part of all Epic EHRs, and it will build off our grant.
Physician Focus: In 2018, you helped launched the Disability Equity Collaborative, a national initiative dedicated to improving healthcare for people with disabilities. What inspired you to start this effort?
Dr. Morris: During our documentation work around disability status more than a decade ago, I started getting calls from health systems. They were overwhelmed by the Affordable Care Act’s mandate that organizations have equity leaders—with a big part of that centering on disability—and also the rising lawsuits from patients over lack of accessibility. Organizations started hiring individuals to be in charge of all disability accessibility, but there’s no manual or blueprint of how to do this. The first thing they need is to document disability. They found my research and started calling me, feeling alone and overwhelmed.
“Organizations started hiring individuals to be in charge of all disability accessibility, but there’s no manual or blueprint of how to do this.”
Recognizing this need for health systems to have direction and support in adopting polices around disability motivated the launch of the Disability Equity Collaborative. Initial funding was provided by the Patient-Centered Outcomes Research Institute (PCORI). We have over 350 different stakeholders involved, including a learning collaborative with representation from almost 300 hospitals from across the country.
It’s an opportunity for organizations to get together to share challenges, successes, and resources. The Joint Commission, U.S. Government Accountability Office, and multiple groups within the Centers for Medicare & Medicaid Services often come to us for feedback or input from our group of health systems. This group is for supporting health systems, but I feel like we’ve been able to have a larger impact on policy and practice.
Physician Focus: You’ve also led studies to help highlight inequitable care for people with disabilities. Can you tell us about this work?
Dr. Morris: Right now, it’s very descriptive work. We’re talking with patients and clinicians. For one study, we surveyed medical students and also gave them the Implicit Association Test (IAT) and were able to demonstrate the existence of biases around disabilities.
For another study that we recently finished, funded by a $4.3 million grant from PCORI, we developed a tool to improve the quality of communication between patients with communication-related disabilities—speech, language, voice, and hearing disabilities—and their primary care providers. We had 16 strategies that patients would benefit from. Each patient would pick their top three strategies, like “I need you to look at me while you’re speaking,” and then bring that into the clinical encounter to share with the clinician. In our randomized controlled trial, we found that the tool did improve some communication outcomes: the main one was the patients’ feeling of being respected by their clinician.
Physician Focus: What other initiatives are you working on now?
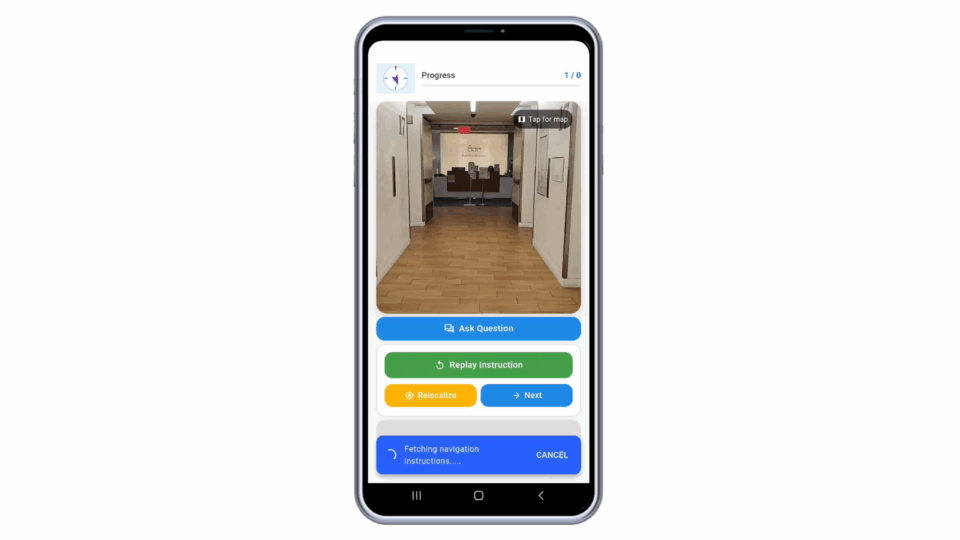
Dr. Morris: John-Ross Rizzo, MD, and I are co-PIs on an NIH ableism grant around improving the accessibility of healthcare for people who are blind and low vision. Specifically, we’re working with Perlmutter Cancer Center’s Beatrice W. Welters Breast Health Outreach and Navigation Program to modify patient navigation for people who are blind or have low vision to make sure they have the supports they need to access care.
Related to this, our Disability Equity Collaborative is building out a tool kit for health systems with people with disabilities. It will have all kinds of resources and supports for organizations, from how to set up an accessibility program from the beginning stages to more specifics on different accessibility initiatives in the organization. I’m resubmitting an R01 grant to test this tool kit in a randomized controlled trial.
We also hope to conduct a large-scale trial to compare different models of the disability coordinator role, which is still ill-defined. I think we have the opportunity to really set the standard and define what this is in the U.S. healthcare system.