
Upwards of 80 percent of Whipple procedures at NYU Langone Hospital—Long Island are performed robotically, a sharp rise from just a few years ago when the medical center first offered the robotic approach. The rapid growth positions NYU Langone Health as one of just a few centers across the nation executing a high-volume robotic Whipple program.
“We have raised our level of performance such that every person who’s eligible for a robotic Whipple, however complex, is able to get one,” says Megan D. Winner, MD, director of the Robotic Surgical Oncology Program at NYU Langone Hospital—Long Island and of Research Information Systems at Perlmutter Cancer Center.
The progress reflects the programmatic approach taken by NYU Langone’s integrated hepato-pancreato-biliary surgery team, and Dr. Winner emphasizes collaboration with surgical colleagues across NYU Langone’s campuses, including Eihab Abdelfatah, MD, and John D. Allendorf, MD, in Long Island, and Steven M. Cohen, DO, and Brock Hewitt, MD, MPH, in Manhattan.
“We have raised our level of performance such that every person who’s eligible for a robotic Whipple, however complex, is able to get one.”
Megan D. Winner, MD
According to Dr. Winner, the program’s success can be attributed to many players across NYU Langone who committed in concert, including surgeons, physician assistants (PAs), and members of leadership who purchased additional robotic surgical systems to ensure ample access.
“The best way to do a Whipple efficiently is to engage the PAs who are robotically trained,” Dr. Winner says. “An unnecessarily long operation is not healthy for the patient or surgeon.” At the Long Island campus, procedures are typically completed in 3.5 hours, and patients can return home as early as 3 days following surgery.
Early in adopting the robotic Whipple, Dr. Winner recalls performing on a patient with a tumor in a difficult location, in the posterior uncinate process and above the inferior vena cava. The case reinforced to Dr. Winner the unparalleled operative and postoperative experience offered by the procedure.
“In adopting the robotic Whipple platform, I was worried about compromising any of the excellent quality that we have achieved in our open Whipple program. But what I’ve learned from my patients who went through these procedures is there is tremendous benefit offered by the robotic platform.”
Disclosures
Dr. Winner has participated in courses sponsored by Intuitive Surgical, Inc. but is not a paid consultant for the company.
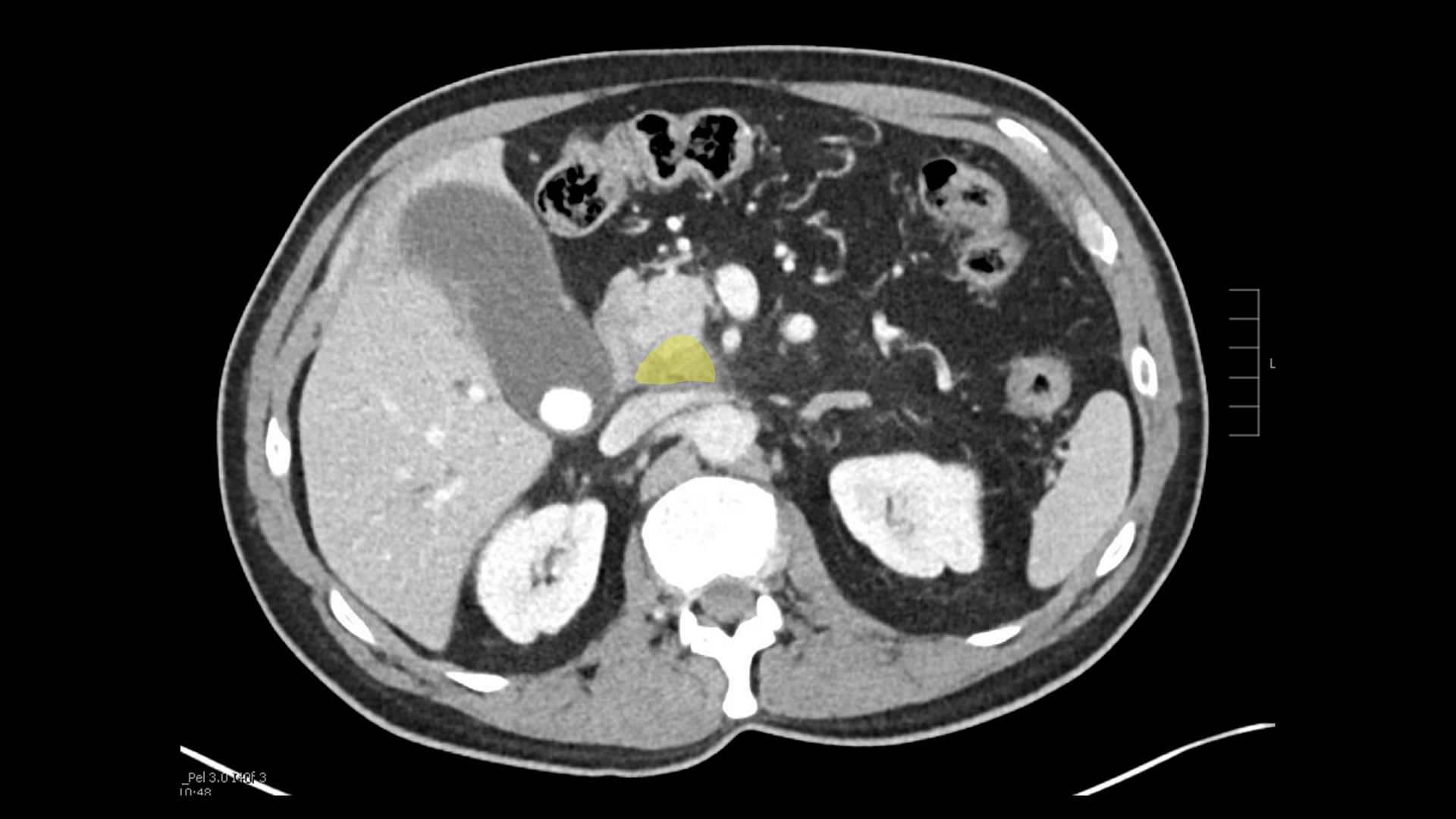
A Tumor Atop the IVC
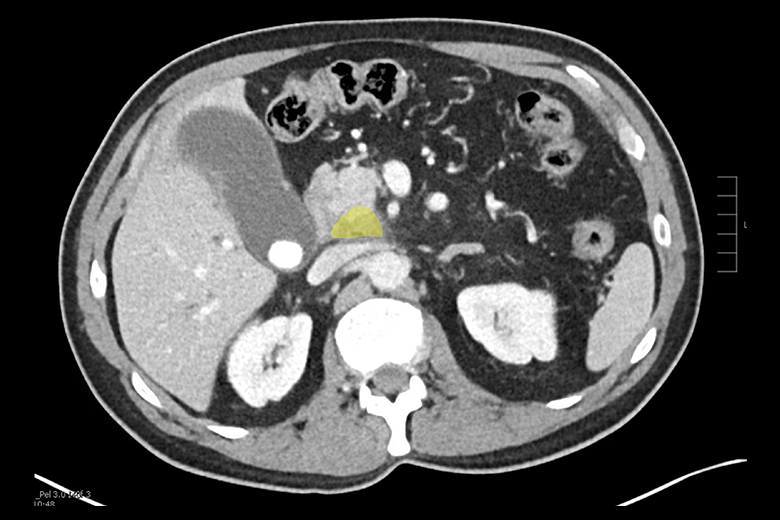
Imaging reveals a pancreatic tumor (yellow) located near the inferior vena cava (IVC).
A 73-year-old patient presented to NYU Langone Health with a pancreatic tumor sitting directly above the IVC. The patient was scheduled for a Whipple and qualified for a robotic approach.
Setting Up for Success
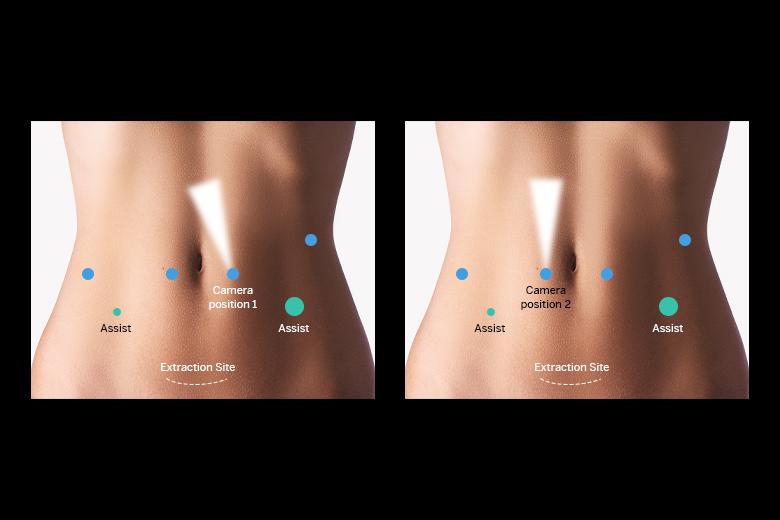
Diagram of port placement. All ports are aligned in a row across the abdomen except one port by the left ribcage is moved up to ensure less interference during key suturing maneuvers.
The success of the robotic approach adopted at NYU Langone starts with patient positioning and port setup. A split-leg position allows the surgical assistant more access to the abdomen, improving efficiency and reducing fatigue. The surgical team emphasizes the benefit of refining port placement and instrument use as the robotic experience grows.
A Clear View of the Critical Anatomy
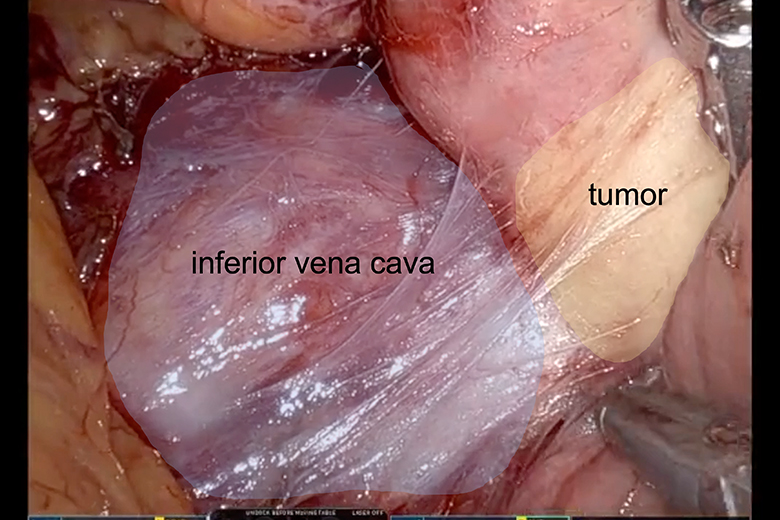
Surgeon’s view, showing the proximity of the tumor (right) to the IVC (left).
Surgeon Megan D. Winner, MD, performed the Whipple, which she typically begins by elevating the colon and dividing the attachments of the duodenum, enabling easier handling of the anatomy when addressing bleeding. Midway through, the camera location is changed from patient left to patient right, improving visualization and minimizing organ traction as the gallbladder is excised and the small bowel is moved away from the colon.
Separating the Tumor from the IVC
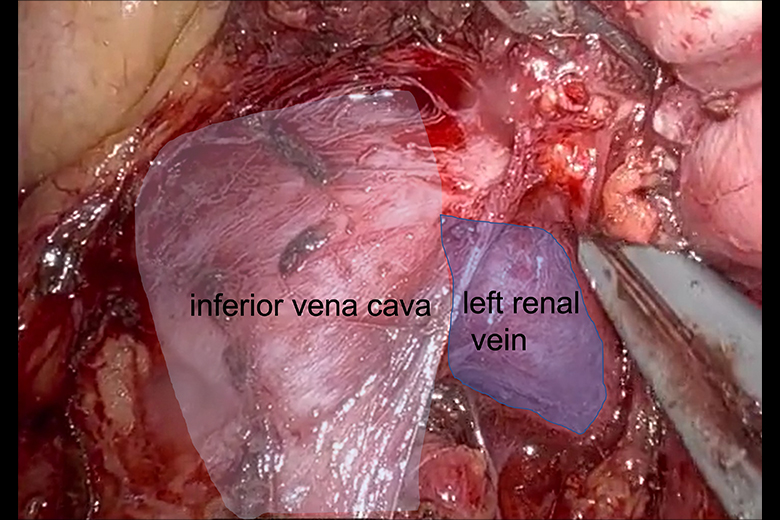
Surgeon’s view, showing the complete dissection of the IVC (left) and the left renal vein (LRV) (right) from underneath the tumor.
Separating the tumor from the IVC at the confluence of the LRV was the most vulnerable operative step. The robotic platform enabled this to be performed with perfect visualization and in a near-bloodless manner, proving superior to an open approach, and secured the ability to proceed with the robotic system. If the vessel had been involved directly, an open operation with reconstruction of the IVC would have been required.
Reconstruction and Recovery
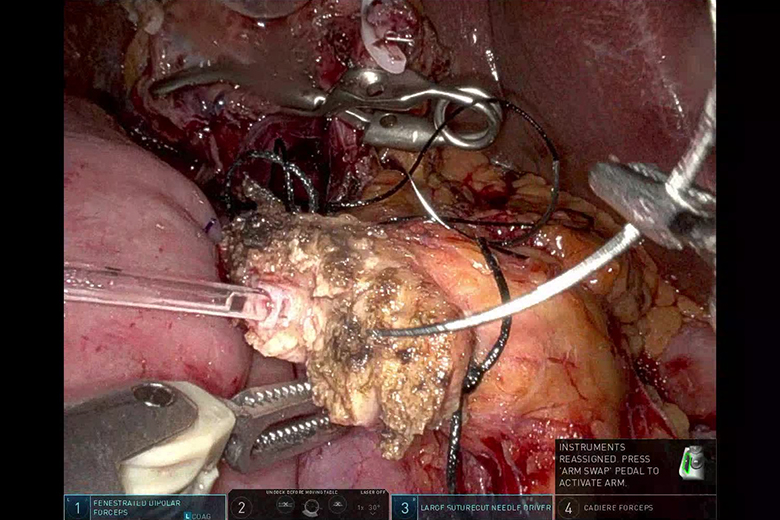
Surgeon’s view during reconstruction and anastomosis following the Whipple procedure.
During reconstruction, a connecting limb is extended below the colon to the pancreas, with another extended above the colon to the stomach, and adipose tissue is interposed. Dr. Winner speculates this separation lessens the impact of a pancreatic anastomosis leak, reduces the occurrence of delayed gastric emptying, shortens the length of stay, and has driven a reduced need for gastronomy tubes. This patient was discharged on postoperative day 4.



