

Posterior shoulder dislocations represent 2 to 4 percent of all shoulder dislocations and are frequently missed or misdiagnosed on initial presentation.1,2 When left unreduced for an extended period of time, these injuries become chronic locked dislocations and are typically associated with an anteromedial impaction fracture of the humeral head that occurs as the humeral head impacts against the posterior glenoid rim—commonly referred to as a reverse Hill-Sachs lesion.1,3,4 The size of these defects often correlates with the chronicity of the dislocation. The longer the dislocation has been present, the larger the impaction fracture and associated compromise of the articular surface.4
Management of these large reverse Hill-Sachs lesions involving 30 to 50 percent of the articular surface remains controversial, as they fall between the threshold for lesser tuberosity transfer (typically less than 30 percent) and arthroplasty (typically greater than 50 percent).5,6
Here, we present a case of a chronic posterior shoulder dislocation with a large reverse Hill-Sachs defect successfully treated with humeral head osteochondral allograft reconstruction with a 13-year follow-up.
Case Highlights:
- A chronic locked posterior shoulder dislocation after seizure activity produced a 40 percent reverse Hill-Sachs defect.
- Humeral head osteochondral allograft reconstruction restored function while preserving the native humeral head.
- At five-month follow-up, the patient had minimal discomfort, forward elevation to 170°, external rotation to 60°, and internal rotation to the posterior ileum.
- At 13-year follow-up, the patient maintained near-normal motion, minimal pain, and only mild degenerative change.
Presentation
A 55-year-old right-hand-dominant man presented approximately one month after sustaining two seizure episodes while traveling abroad, after which he developed persistent pain and marked loss of motion in the left shoulder. He was told to seek the care of an orthopedic surgeon when he returned to the United States.
At the time of initial evaluation, he denied recurrent instability events and reported no numbness or tingling. His medical history was notable for diabetes mellitus, hyperlipidemia, and a seizure disorder. Medications included metformin, simvastatin, and phenytoin. He reported that his seizures had been well controlled until the recent events.
On examination, the left shoulder had mild anterior flattening and mild tenderness globally. Active motion was limited to approximately 70° of forward elevation, external rotation to -45°, and internal rotation to the lumbosacral region, with crepitus and discomfort throughout motion. Deltoid strength was 5/5, external rotation strength was slightly decreased, and axillary nerve sensation and the distal neurovascular examination was unremarkable.
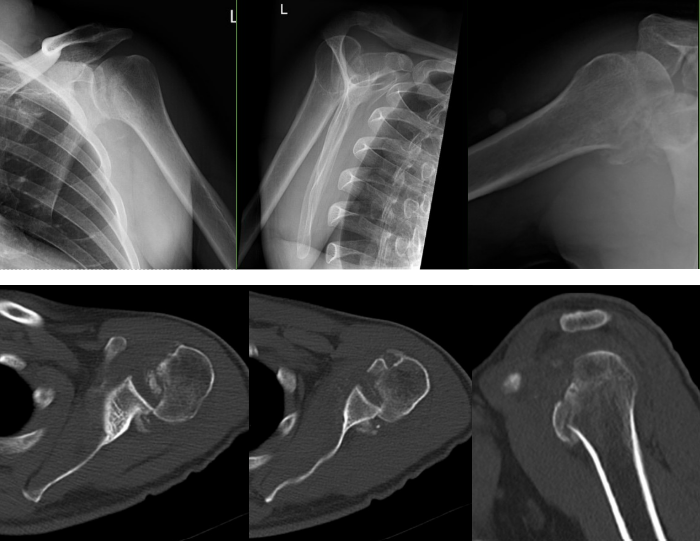
Standard imaging demonstrated a posterior dislocation of the glenohumeral joint with a large reverse Hill-Sachs defect engaged on the posterior glenoid rim (Figure 1). CT scan provided important information about the exact size of the defect, percentage involvement of the articular surface, and any associated damage to the glenoid. Measurements showed that 40 percent of the articular surface was involved.
Different treatment options were discussed, but based on the patient’s age, size of the defect, and the status of the intact articular cartilage, operative management was recommended with a plan for open treatment and a joint-preserving reconstruction using a humeral head osteochondral allograft.
Operative Management
After placement of a regional interscalene block, the patient was placed in the beach chair position. A standard deltopectoral approach was utilized. The conjoined tendon was carefully mobilized off the subscapularis. In chronic dislocations, this is an area of adhesions. The posterior position of the humeral head alters the expected anatomy, so careful dissection is essential.
The subdeltoid and subacromial adhesions are released. The humeral head is in an internally rotated position, so identification of the lesser tuberosity is essential to ensure that the location of the subscapularis tenotomy can be identified 1 cm medially.
After subscapularis tenotomy, the medial edge of the tendon is tagged with sutures, and subcoracoid adhesions are released. Inferior capsular releases allow mobilization of the humerus. Any soft tissue within the glenohumeral joint is removed to expose the locked posterior dislocation.
The humerus is internally rotated, so a Darrach elevator could be inserted between the glenoid and the humeral head. The elevator is then used as a “shoehorn” to reduce the remaining humeral head onto the glenoid. At this point, additional capsular releases are performed to achieve additional external rotation.
The reverse Hill-Sachs defect involved approximately 40 percent of the articular surface, with nonviable cartilage at the base of the defect. The glenoid cartilage and remaining posterior humeral head cartilage were intact. A humeral head osteochondral allograft was contoured to match the wedge-shaped defect and provisionally stabilized with Kirschner wires. Definitive fixation was achieved with two countersunk 4.0-mm cancellous screws (20 mm and 45 mm) (Figures 2 and 3).
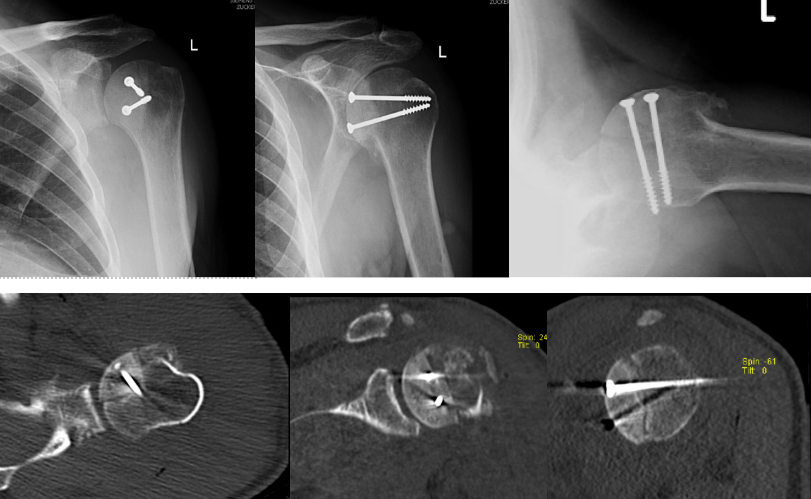
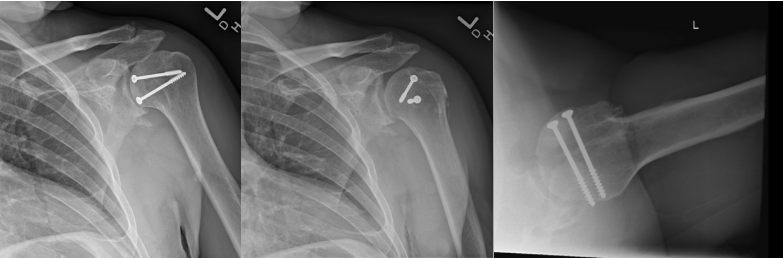
After fixation, the construct was stable throughout range of motion, restoring articular congruity. The subscapularis and rotator interval were repaired, and the patient was placed into a gunslinger shoulder immobilizer postoperatively.
Postoperative Course
The patient was maintained in the gunslinger orthosis and evaluated at regular intervals postoperatively. He began passive range of motion exercises above the position of the orthosis at the two-week visit, allowing for forward elevation to 100° and external rotation to neutral. Formal physical therapy began at approximately one month, when the orthosis was discontinued.
At the five-month follow-up, the patient had minimal discomfort. On examination, he had active forward elevation to 170°, external rotation to 60°, and internal rotation to the posterior ileum.
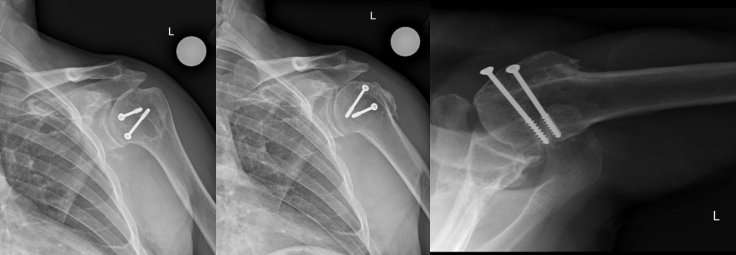
He was most recently evaluated at 13-years after the procedure. The patient reported high satisfaction and independent function, with only mild pain at maximal cross-body adduction. Examination showed a well-healed incision, active forward elevation to 170°, external rotation to 40°, and internal rotation to the lumbosacral junction with full strength of the deltoid and rotator cuff. Radiographs demonstrated a well-healed humeral head allograft, mild glenohumeral degenerative changes, a maintained subacromial space, and a centered humeral head on both anteroposterior and axillary views (Figure 4).
Discussion
Multiple joint-preserving surgical techniques have been described for treating large reverse Hill-Sachs defects, including the McLaughlin and modified McLaughlin procedures and arthroscopic subscapularis remplissage.2,7,8,9,10,11 However, segmental humeral head reconstruction with osteochondral allograft represents an alternative approach that aims to restore native anatomy and articular congruity while preserving the native humeral head.5,6
Gerber and Lambert12 first described this technique in 1996, reporting successful allograft reconstruction in four patients with defects of at least 40 percent of the articular surface, with stability maintained at an average follow-up of 68 months.
Gerber et al.13 further reported on the long-term outcomes of this same technique. Of the 22 shoulders treated with allograft reconstruction for defects involving at least 30 percent (mean 43 percent) of the humeral head, at a mean follow-up of 128 months, 18 of 19 shoulders were rated as subjectively excellent. Only two patients required conversion to arthroplasty over 15 years after the initial allograft reconstruction procedure.
Similarly, Marcheggiani Muccioli et al.5 demonstrated favorable mid-term results with fresh-frozen humeral head allografts, reporting mean Constant-Murley scores of 82 points, minimal osteoarthritis development, and an average allograft resorption rate of only 4 percent with no failures at 66 months follow-up.
Compared to other methods of addressing humeral head defects, osteochondral allograft offers the advantage of restoring the native articular surface rather than filling the defect with non-articular tissue, which may be particularly beneficial in younger, active patients seeking to preserve long-term joint function.
Our patient, at 13-years post operatively, continues to report high satisfaction, preserved motion, with minimal pain.
References:
- Saupe N, et al. Radiology. 2008;248(1):185-193. DOI
- Haritinian EG, et al. BMC Musculoskelet Disord. 2023;24(1):82. DOI.
- Yang K, et al. J Shoulder Elbow Surg. 2025;34(1):88-95. DOI.
- Moroder P, et al. Am J Sports Med. 2016;44(3):708-714. DOI.
- Marcheggiani Muccioli GM, et al. BMC Musculoskelet Disord. 2021;22(1):768. DOI.
- Saltzman BM, et al. Arthroscopy. 2015;31(9):1827-1834. DOI.
- Martetschläger F, et al. Knee Surg Sports Traumatol Arthrosc. 2013;21(5):1189-1194. DOI.
- Xiong F, et al. BMC Musculoskelet Disord. 2023;24(1):114. DOI.
- Romano AM, et al. Knee Surg Sports Traumatol Arthrosc. 2021;29(7):2348-2355. DOI.
- Cohen M, et al. J Shoulder Elbow Surg. 2022;31(1):100-106. DOI.
- Konda SR, et al. J Orthop Trauma. 2017;31(Suppl 3):S36-S37. DOI.
- Gerber C, Lambert SM. J Bone Joint Surg Am. 1996;78(3):376-382. DOI.
- Gerber C, et al. J Shoulder Elbow Surg. 2014;23(11):1682-1690. DOI.

