A Multiplex Approach to Facial Reanimation
For patients with partial or total facial paralysis, surgeons at NYU Langone Health have developed a new approach to facial reanimation. The approach connects distal branches of the facial nerve to multiple local and regional nerves to improve segmented movement.
Traditionally, either the main trunk or a single division of the facial nerve is attached to a single nerve for reanimation, which can result in mass movement (synkinesis). This oversimplified approach does not account for the way the facial nerve divides and segments across five distinct facial areas, says Adam S. Jacobson, MD, chief of the Division of Head and Neck Surgery. “To me, it never made sense to graft the main facial nerve together and expect it to perform the same way, with signals reaching their rightful places.”
Jacobson and colleagues including Jamie P. Levine, MD, chief of microsurgery, and Judy W. Lee, MD, director of the Facial Paralysis and Reanimation Center, developed the multigraft technique to offer surgeons a more consistent, nuanced approach to facial reanimation.
Says Dr. Levine, “We’re giving multiple inputs to the damaged nerves, so over time they start sequentially taking over and giving different levels of control to the segments of the face.”
“Our technique offers an immediate solution rather than a wait-and-see approach.”
Adam S. Jacobson, MD
Each harvested nerve is selected based upon the needs of each facial region, Dr. Levine adds. “For example, the ansa cervicalis offers tone to the vocal chords, so we’re using it in the eyes—an area where we wanted tone. For the midface division, we needed power, and looked to the masseteric nerve.”
The new technique reduces mass facial movements which can have life-altering effects for patients. “Our technique offers an immediate solution rather than a wait-and-see approach or the traditional facial reanimation approach,” Dr. Jacobson says. “The sooner a nerve transfer surgery is performed, the better the functional outcomes.”
Enhanced Segmented Movement via Multiple Grafts

A patient demonstrating left facial paralysis.
A new approach to facial reanimation developed by surgeons at NYU Langone Health connects distal branches of the facial nerve to multiple local and regional nerves. The technique is applicable for patients with abnormal nerve growth, such as those with Bell’s palsy, or patients with nerve loss whether due to a degenerative condition or prior surgery. Here, a patient demonstrates left facial paralysis possibly due to a genicular ganglion hemangioma.
Up to Four Distinct Nerve Connections
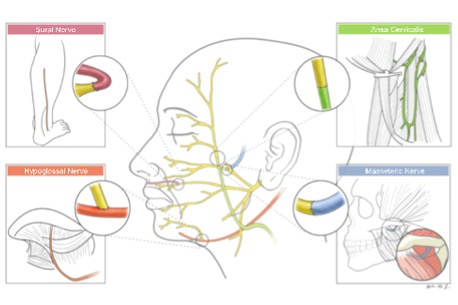
Illustration depicting four possible nerve connections utilized in the new multigraft facial reanimation approach. IMAGE: Andrew Lee, MD, artist.
The masseteric nerve is connected to the distal end of the midface division. The lower division of the facial nerve is connected to the hypoglossal nerve to animate the lower face. The ansa cervicalis is connected to the upper division of the face to give tone to the eye muscles. A cross-face nerve graft may be used to innervate the affected midface with input from the intact contralateral midface division.
Rapid Functional Improvement
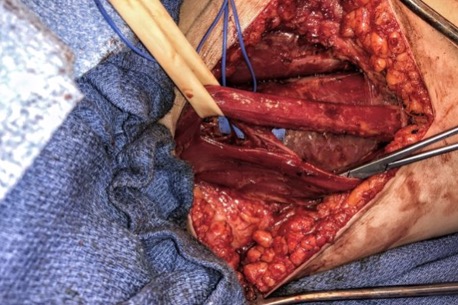
Surgeon’s view during a nerve graft procedure.
The nuanced reconstruction technique requires muscular transfer or transplant and takes longer than traditional facial reanimation techniques as each nerve is transferred and carefully grafted. However, surgeons have not observed significantly longer patient recovery times, with most patients experiencing some functional recovery 3–12 months after surgery.
Facial Reanimation with Less Synkinesis

A patient demonstrating segmented movement following multigraft facial reanimation to address left facial paralysis.
Patients benefit from facial reinnervation that enables specialized movement, with less synkinesis than traditional single-graft techniques. Here, the patient who experienced left facial paralysis demonstrates segmented movement made possible by the multigraft technique. Follow-up photos were taken two years post-surgery.