
A Rare, Yet Catastrophic Injury
A pediatric patient with Erb’s palsy experienced a remarkable recovery after specialists at NYU Langone Health teamed up to perform early microsurgical reconstruction and intensive occupational therapy. The patient first presented to the pediatric orthopedic hand surgery clinic at Hassenfeld Children’s Hospital for evaluation of her right upper extremity by Andrew E. Price, MD and Jacques H. Hacquebord, MD, attending surgeons on the case.
“Brachial plexus birth injuries require a team of highly specialized experts, including surgeons and occupational therapists,” says Dr. Price. “After birth, these injuries are usually treated conservatively using custom splints, electrical stimulation, and occupational therapy—we’re one of the few centers capable of doing all three.”
“These injuries are usually treated conservatively using custom splints, electrical stimulation, and occupational therapy—we’re one of the few centers capable of doing all three.”
Andrew E. Price, MD
Despite conservative management, the patient failed to regain biceps function at 6 months of age. The best treatment was determined to be brachial plexus neurolysis with double fascicular nerve transfer. Dr. Price, Dr. Hacquebord, and their team also injected botulinum toxin into several antagonist muscle groups during the procedure to improve shoulder and elbow motion.
“The prognosis of Erb’s palsy depends on several factors including the extent of the injury, size and severity of the post-ganglion tears, speed of recovery, and quality of initial treatment,” says pediatric occupational therapist Lori B. Ragni, MS, OTR/L. “While surgical repair is not always needed, in the right setting it will enable better functional outcomes, especially when combined with occupational therapy.”
“While surgical repair is not always needed, in the right setting it will enable better functional outcomes, especially when combined with occupational therapy.”
Lori B. Ragni, MS, OTR/L
Upon discharge, the patient continued outpatient rehabilitation with Rusk Rehabilitation. Two years after surgery, the patient is doing extremely well, with sustained improvements in several clinical and functional outcomes.
Preoperative Diagnosis: Injury of Right Brachial Plexus
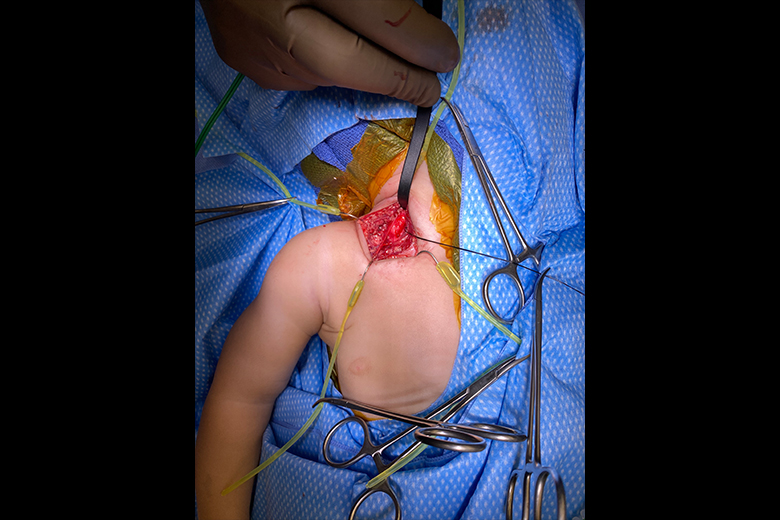
Surgeon’s view of a large neuroma in the neck of an infant.
The patient’s right upper extremity was held with shoulder internally rotated, elbow extended, wrist flexed, and forearm pronated. She demonstrated excellent triceps strength but had no biceps function. Moreover, she did not exhibit shoulder elevation or active wrist extension. The patient was referred for occupational therapy and splinting, with surgery ultimately deemed necessary.
A Successful Surgery
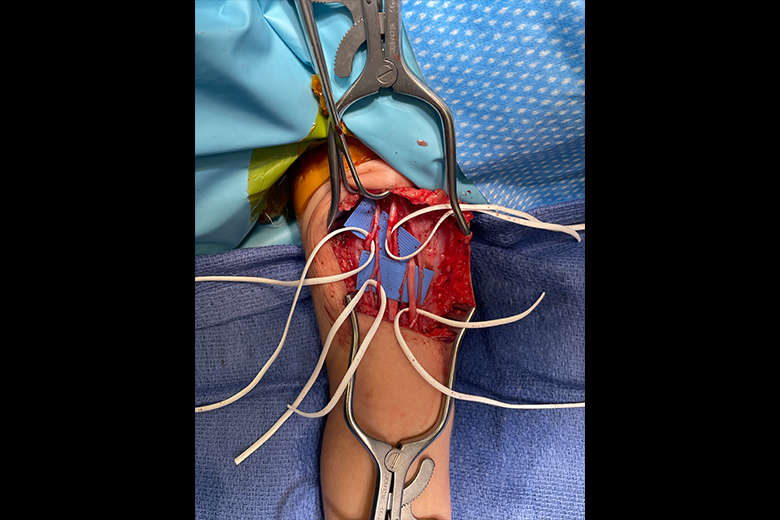
Surgeon’s view while identifying nerves in the patient’s arm.
Upon exploration of the right brachial plexus, the C6 nerve was found to have significant scarring and lack of stimulus conduction. There was contractility of the deltoid with stimulation at 2 mA of C5 proximally, but no contractility with stimulation of C6. The team proceeded with the procedure that included neurolysis of the brachial plexus and double fascicular nerve transfer.
Long-Term Outpatient Rehabilitation
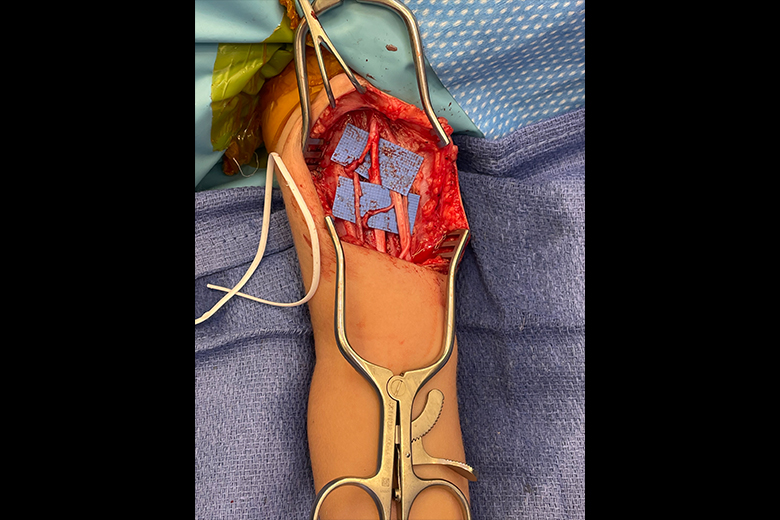
Surgeon’s view of nerves in the patient’s arm after transfer.
At 2-year follow-up, the patient demonstrated significant improvement. She had regained shoulder elevation to above 130 degrees, full passive shoulder external rotation, negative clarion, active elbow flexion, supination to 10 degrees, no elbow flexion contracture, and some active extension of the wrist.





