
Patient interest in kidney-sparing treatment options for upper tract urothelial carcinoma (UTUC) is growing. At NYU Langone Health, we have seen excellent success with one such treatment, chemoablation with UGN-101 (Jelmyto), and treat a large number of patients with the agent.
In this Case of the Month, we present an elderly patient with a low-grade UTUC obstructing her only remaining kidney. Over a decade earlier, she had undergone a nephroureterectomy for the disease, but now faced a new primary tumor threatening her renal function and raising the possibility of dialysis. Hoping to avoid such an outcome, she sought alternatives to surgery that could preserve her quality of life.
Her case underscores the important role of innovative therapies that provide patients the chance to spare their kidney.
Case Highlights:
- A 91-year-old female with a history of UTUC and prior left nephroureterectomy presented with a tumor obstructing her right ureter.
- She underwent endoscopic resection to preserve her remaining kidney, followed by UGN-101 induction to reduce recurrence risk.
- She remains recurrence-free over 18 months later.
- At NYU Langone, UGN-101 is widely used, with around 10 percent of cases involving patients with a single kidney.
Patient Case
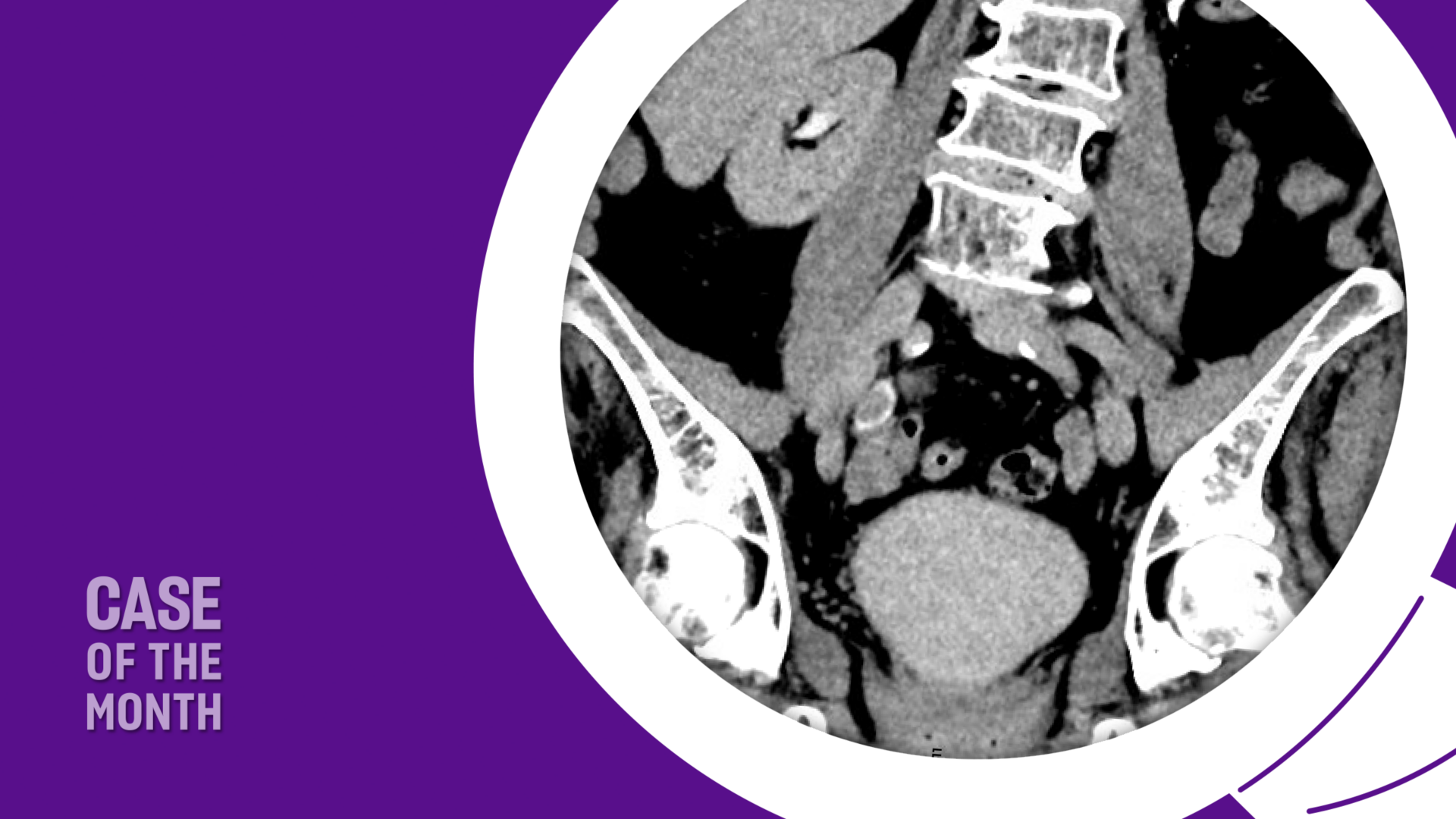
The 91-year-old female patient was healthy and functional, with a history of upper tract urothelial carcinoma (UTUC). Over 11 years ago, she underwent a left nephroureterectomy for this disease. Unfortunately, due to the recurrent manner of UTUC and the metachronous occurrence, she presented now with a low-grade tumor obstructing her remaining kidney. The tumor was located in the ureter on the right side (Figure 1) and she was experiencing a slight decline in her renal function. She wanted to avoid dialysis, which would be necessary if her kidney were to be removed.

We performed a ureteroscopy with laser resection of the ureteral tumor and complete visual removal of the mass. A ureteral stent was left in place after surgery to prevent any ureteral stricture from the area of the laser ablation.
The patient had a strong understanding of the disease and recognized the risk of recurrence to be upward of 60 percent or even higher in some reports. The patient expressed ongoing worry about her age, which made further surgical resections and ablations less ideal. At this point, we discussed Jelmyto, a reverse thermal hydrogel installation of mitomycin. The gel is liquid at low temperatures, allowing it to be easily instilled via a catheter, and it solidifies at body temperature, enabling prolonged local drug exposure to the tumor site. It is typically administered once weekly for six weeks.
In the first experiences with this formulation in a real-world setting, the complete response rate of the cancer after a complete endoscopic ablation was over 75 percent in patients with low-grade UTUC.1 Long-term data is not yet published, but at the American Urological Association’s 2024 annual meeting, an abstract was presented on this topic: in those patients who had a complete response after UGN-101 induction, the median survival was not reached, and recurrence-free survival at 24 months was over 85 percent.2
For our elderly patient seeking options to improve her overall quality of life, the results have been very similar. After complete endoscopic tumor removal and induction UGN-101, she has remained recurrence-free for over 18 months.
Discussion
UGN-101 was approved in early 2020, and since then its use for low-grade UTUC has continued to grow in the United States. At NYU Langone, we offer it alongside other new therapies for patients with all disease states. The experience has been positive and has been widely adopted by all urological oncologists and endourologists within the Department of Urology. Roughly 10 percent of our UGN-101 treatments are for patients with a single remaining kidney.
In the case presented, a patient with one kidney sought to avoid a rigorous dialysis regimen in her remaining years. Tumor resection made this possible, while UGN-101 helped address her concerns about recurrence.
To support informed treatment decisions, the American Urological Association released its first UTUC guidelines in 2023.3 The resource allows for risk stratification and the judicious use of aggressive treatments for high-risk disease and less-aggressive therapies and interventions for low-risk disease.
References
