Case Highlights:
- A patient under 5 with cerebral palsy presented with a hip subluxation of 55 percent, typically indicating osteotomy, but the family sought options that minimized risk of blood transfusion.
- Outpatient proximal femoral guided growth was performed, using a single screw to guide the femur to grow into a more varus position and gradually correct hip subluxation.
- Two years after surgery, the hip dysplasia has been corrected, and no further intervention is likely needed.
- Routine orthopedic screening every 6 to 12 months beginning at age 2 is key to early detection of hip dysplasia in children with cerebral palsy and successful treatment with guided growth.
In the fall of 2023, a patient under 5 years old with spastic hemiplegic cerebral palsy and progressive right hip subluxation was referred to Mara Karamitopoulos, MD, MPH, chief of the Division of Pediatric Orthopedic Surgery at Hassenfeld Children’s Hospital at NYU Langone, for a second opinion.
Over the previous six months, the patient had experienced a growth spurt, with hip subluxation rapidly progressing from 15 to 55 percent. An outside institution recommended a traditional varus derotation osteotomy, but the parents wanted to avoid any surgery that carried even a small risk of requiring a blood transfusion.
At NYU Langone, Dr. Karamitopoulos presented them with an alternative: proximal femoral guided growth. This newer, less invasive surgery is performed over a guidewire with minimal to no blood loss and is currently only offered at select pediatric orthopedic programs across the US.
“As early adopters, we routinely offer this technique to eligible patients.”
Mara Karamitopoulos, MD
“Guided growth reduces a significant surgery with a hospital stay of three to five days to a 30-minute outpatient procedure,” Dr. Karamitopoulos says. “As early adopters, we routinely offer this technique to eligible patients. It’s another tool that adds to our multidisciplinary care for children with cerebral palsy and neuromuscular hip dysplasia.”
Effective Outpatient Intervention
In the spring of 2024, Dr. Karamitopoulos performed the guided growth procedure under fluoroscopic guidance. After a small incision was made, the procedure was completed over a guidewire. A hip arthrogram was used to visualize the contour of the femoral head and allow for optimal screw length. A 5 mm titanium screw was then placed over the guidewire and advanced across the proximal femoral physis and into the epiphysis. The screw was measured intraoperatively to accommodate future growth.
“The patient was in the post-anesthesia care unit for about an hour, ate an ice pop, and went home the same day,” Dr. Karamitopoulos says. “Most patients take a few doses of ibuprofen or acetaminophen, but otherwise there is essentially no pain.”
“Guided growth reduces a significant surgery with a hospital stay of three to five days to a 30-minute outpatient procedure.”
Patients can bear weight immediately, as this patient did by walking. After two to three days of recovery, most patients can return to school and begin physical therapy.
The screw typically remains in place for one to two years before being removed, allowing the growth plate to resume normal development. Some patients may require a screw exchange 12 to 18 months after surgery to accommodate their physical development.
“We’ll reach that two-year mark in a few months and anticipate being able to remove the screw altogether,” Dr. Karamitopoulos says. “We will keep an eye on his hip as he grows. If it continues to look great, hopefully he will never need to have anything else done.”
Careful Patient Selection and Timing
While proximal femoral guided growth can be performed in children with cerebral palsy as young as 18 months, patients between ages 2 to 7 generally achieve the best outcomes, Dr. Karamitopoulos says.
“For appropriately selected patients, the success rate of guided growth is 90 percent, meaning a varus derotation osteotomy is never needed,” Dr. Karamitopoulos says. “In other patients, guided growth can be a temporizing measure to get them to 6 to 10 years old. If a varus derotation osteotomy is needed, older children and teens tend to tolerate it better than young children. The implants fit better and there are more options for therapy.”

Preoperative X-ray of the patient’s right hip subluxation, which progressed from 15 to 55 percent over six months. Source: NYU Langone Health
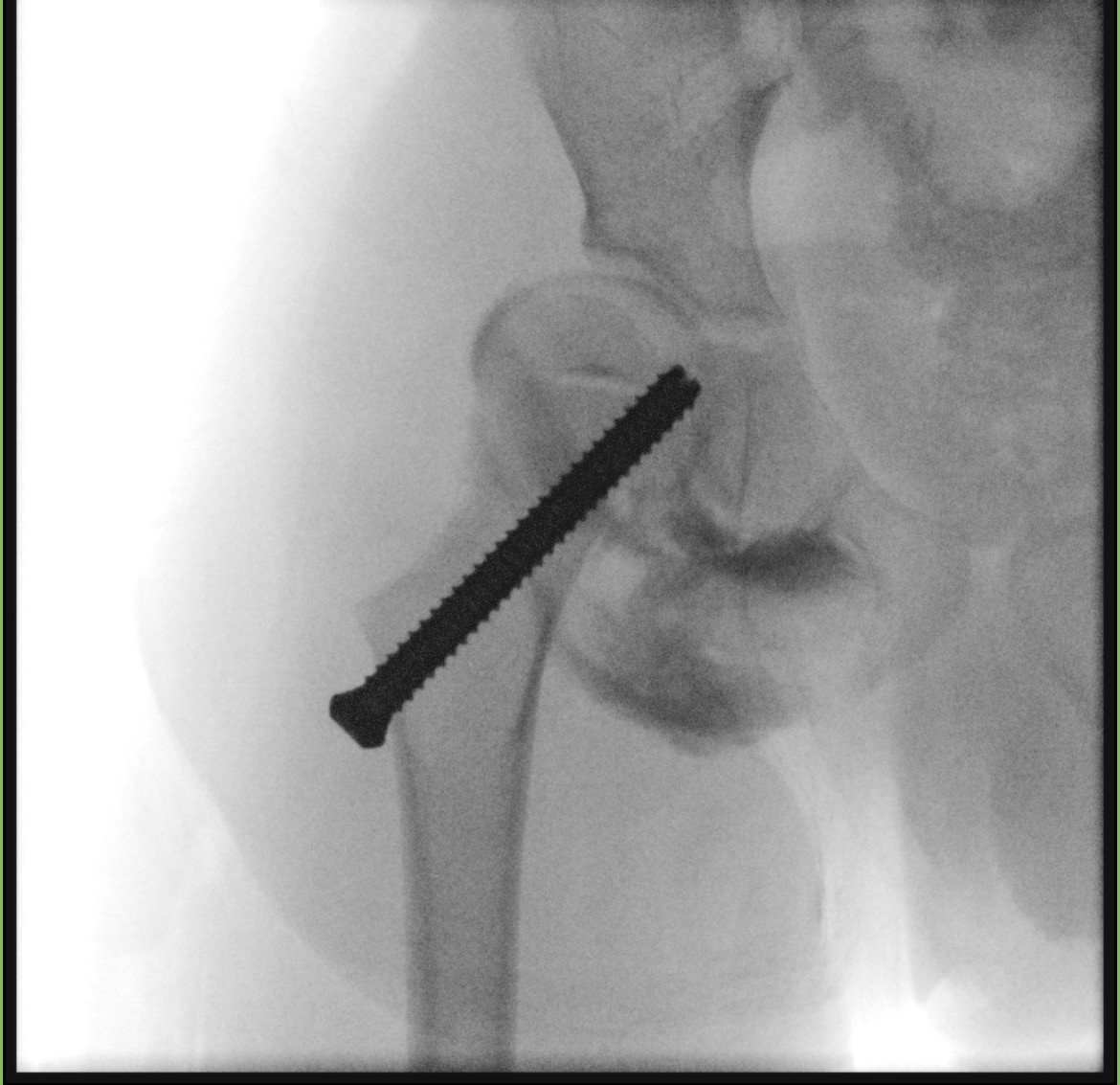
Intraoperative image showing placement of a 5 mm titanium screw during proximal femoral guided growth surgery. Source: NYU Langone Health
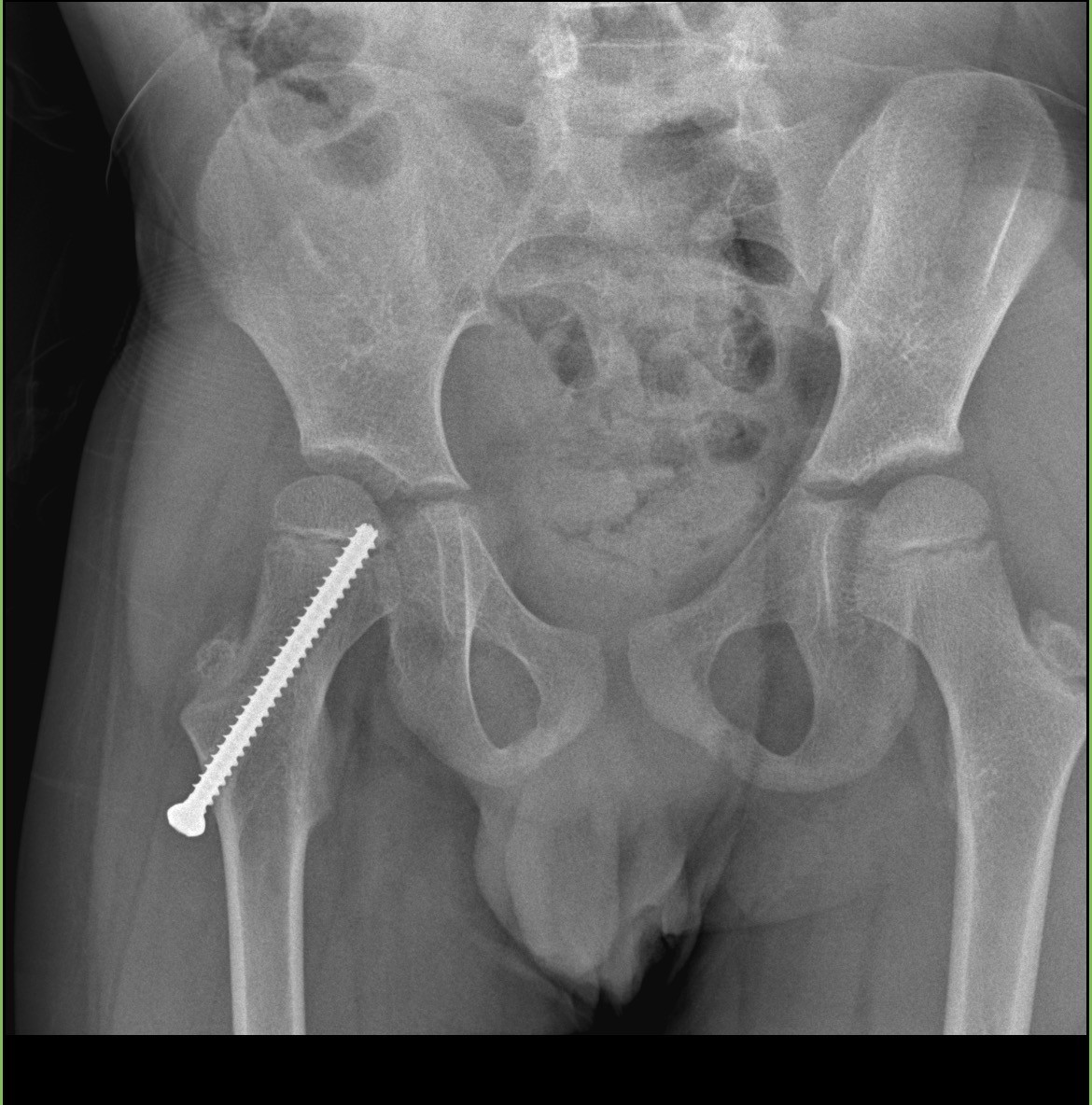
Postoperative X-ray showing screw placement and improvement of the patient’s hip subluxation following guided growth surgery. Source: NYU Langone Health