

For an open fracture or neurovascular injury to an extremity that requires definitive soft tissue coverage through a flap, orthopedic researchers have agreed that it’s best to perform a free flap reconstruction as soon as possible.
In reality, however, scheduling and other conflicts can delay the time to coverage. Some surgeons have maintained that improved technology has lessened the urgency. Others have pointed to the potential existence of a temporary “inflammatory period” during which reconstruction should be avoided. Within this time frame, it’s proposed that irritated blood vessels may heighten the risk of thrombosis and surgical failure.
A systematic review and meta-analysis led by orthopedic surgeon Jacques Hacquebord, MD, and colleagues at NYU Langone Health support the general consensus that immediate reconstruction within three days is most effective. Beyond that window, however, the study has suggested a relatively nonlinear relationship between time and outcomes.
“Get to free flap reconstruction as early as possible: the evidence is very strong that less than three days is important.”
Jacques H. Hacquebord, MD
“The most objective advice I can give other surgeons is get to free flap reconstruction as early as possible: the evidence is very strong that less than three days is important,” says Dr. Hacquebord, co-director of the multidisciplinary Center for Amputation Reconstruction.
A Matter of Time
Over 1,400 free flap reconstructions from 21 qualifying studies were included in the analyses. “One big takeaway is that the relationship between time and outcomes is nuanced,” Dr. Hacquebord says. “It’s not just the longer you wait, the worse the outcome.”
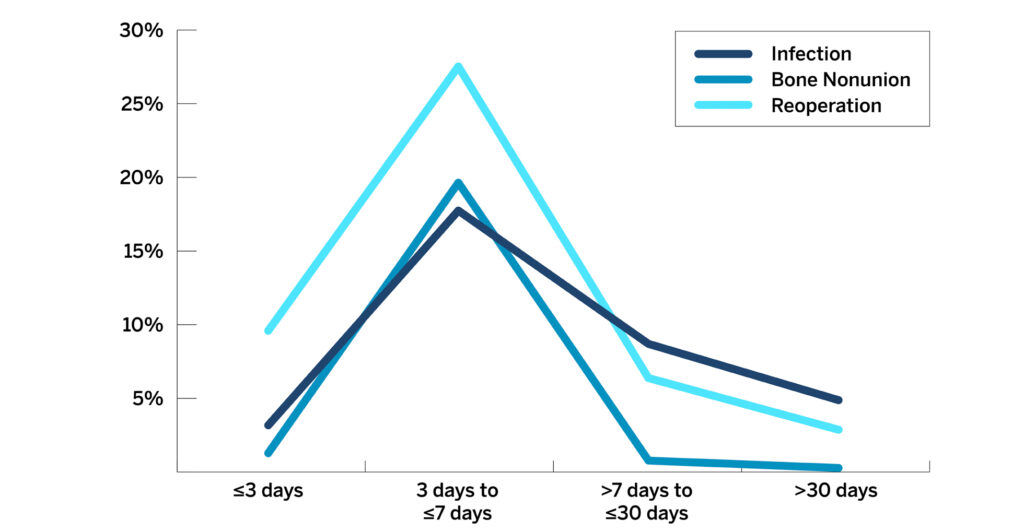
Reconstructions performed between three and seven days after injuries showed significantly higher rates of infections, bone nonunions, and reoperations than did reconstructions done outside this window (Figure 1).
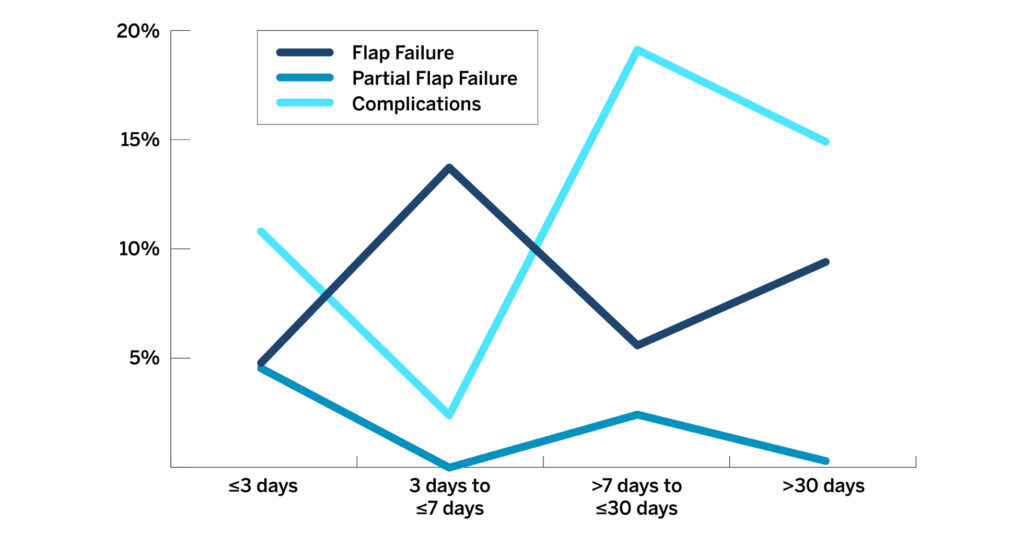
By contrast, no clear trends were observed for rates of flap failure, partial flap failure, and other complications (Figure 2).
In addition, the study showed no significant differences in reconstructions performed between 7 to 30 days or after 30 days postinjury.
Further Research Required
Dr. Hacquebord cautions that more investigation is needed to fully understand the implications of these findings for surgical interventions occurring after the three-day window.
“What we can say is that the middle window of time is associated with a higher rate of infection, bone nonunion, and reoperation,” he says. More-granular studies of the time to coverage and patient outcomes and complications could clarify whether an “inflammatory period” or other factors are contributing to the difference.
For surgeries that cannot occur within that three-day window, he advises optimizing the patients and paying close attention to all intraoperative and postoperative findings as they relate to time.



