
Case Highlights:
- The patient’s skull base osteomyelitis progressed despite prolonged IV antibiotics, with cranial nerve involvement.
- An endoscopic endonasal approach was performed, including partial clivectomy for debridement of infected bone.
- The corridor enabled inset of an ALT free flap for reconstruction.
- The team offers endoscopic endonasal ALT free flap reconstruction of the skull base in select patients, including those with prior treatment for nasopharyngeal cancer.
A man in his late 70s was referred to Carlos D. Pinheiro Neto, MD, PhD, endoscopic skull base surgeon and vice chair of otolaryngology—head and neck surgery at NYU Langone Health, for urgent, advanced management of complex skull base osteomyelitis. The infection involved the nasopharynx, clivus, petroclival junction, and petrous apex on the left side and also impacted multiple cranial nerves, resulting in dysarthria, dysphagia, and intense pain, with rapid deterioration of his overall condition.
The patient’s extensive medical and surgical history—which included several cardiac and metabolic conditions, left mastoiditis and facial palsy, Lemierre’s syndrome, and cervical myelopathy—complicated the case.
Prior to referral in May 2025, he was receiving care at a local hospital with long-term intravenous antibiotics. After several months of treatment without improvement and with worsening symptoms, it was deemed that surgical intervention may be warranted.
“Whenever our team feels we can safely advance novel endoscopic endonasal approaches, we pursue them in the best interest of our patients.”
Carlos D. Pinheiro Neto, MD, PhD
At that time, Dr. Pinheiro Neto discussed endoscopic endonasal cranial base resection to debride the infected bone from the skull base, followed by reconstruction of the cranial base defect with an anterolateral thigh (ALT) free flap. Chandra Sen, MD, the Bergman Family Professor of Skull Base Surgery in the Department of Neurosurgery, and Lindsey E. Moses, MD, a clinical assistant professor of otolaryngology—head and neck surgery, collaborated on the case.
Endoscopic Endonasal ALT Flap Repair
According to Dr. Pinheiro Neto, using an endoscopic endonasal approach for ALT free flap reconstruction of the skull base has been performed in at least six cases to date—all with positive results, and all managed by the multidisciplinary team at NYU Langone Otolaryngology Associates.
“Whenever our team feels we can safely advance novel endoscopic endonasal approaches, we pursue them in the best interest of our patients,” says Dr. Pinheiro Neto. “The benefits to patients, including reduced morbidity, faster recovery, and improved cosmetic outcomes, are substantial compared to open transfacial approaches.”
The ALT free flap was chosen because the patient’s nasoseptal tissue—the traditional source for a local flap in skull base reconstruction—was not adequate for transfer. The surgical team also offers the novel approach to patients with a history of nasopharynx cancer treated with chemotherapy and/or radiation, as these treatments can damage the blood supply of nasoseptal tissue or create defects that may be too complex for local mucosal flaps.
“Vascularized muscle flaps enable the robust delivery of oxygen and nutrients to the wound, which speeds the healing process, especially in the setting of an infection,” says Dr. Pinheiro Neto.
“Drs. Pinheiro Neto and Sen created a very large corridor in the nose, enabling me to insert the ALT flap.”
Lindsey E. Moses, MD
“Drs. Pinheiro Neto and Sen created a very large corridor in the nose, enabling me to insert the ALT flap,” Dr. Moses says, “after which I connected a blood supply to the flap by tunneling to an artery and vein in the neck—it was a success.”
Surgical Approach and Debridement
To address the infection prior to reconstruction, the team performed an endoscopic endonasal approach to the ventral skull, including total ethmoidectomy, sphenoidotomies, posterior septectomy, right medial maxillectomy, and midline nasopharyngectomy. They also performed a partial clivectomy for resection of the infectious process involving the clivus and left petroclival junction.
“Successfully navigating the nasal passages endoscopically proved to be the most technically challenging part of the surgery.”
Chandra Sen, MD
“Successfully navigating the nasal passages endoscopically proved to be the most technically challenging part of the surgery,” Dr. Sen says. “The infection had spread across the skull base and was starting to impact several cranial nerves.”
Overall, the procedure was a success, with resolution of infection within six weeks and marked improvement in the patient’s function. The patient also received vocal cord injections under the direction of Milan R. Amin, MD, which improved his speech and vocal quality.
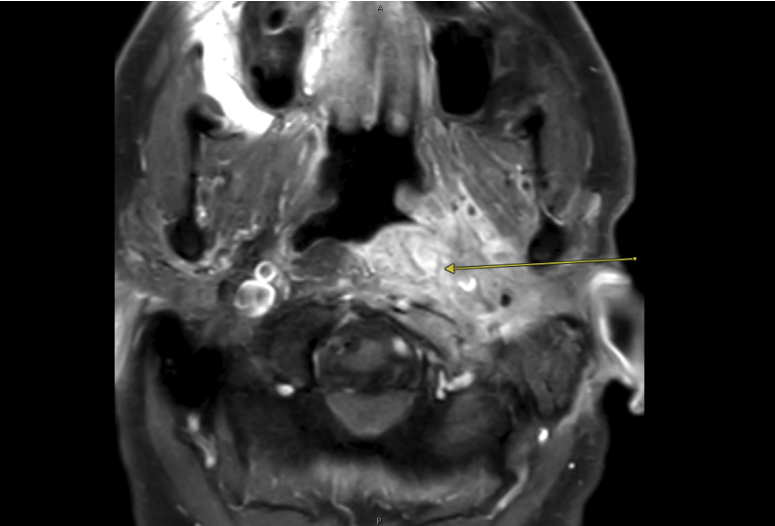
MRI showing the extensive skull base infection (arrow). Source: NYU Langone Health.
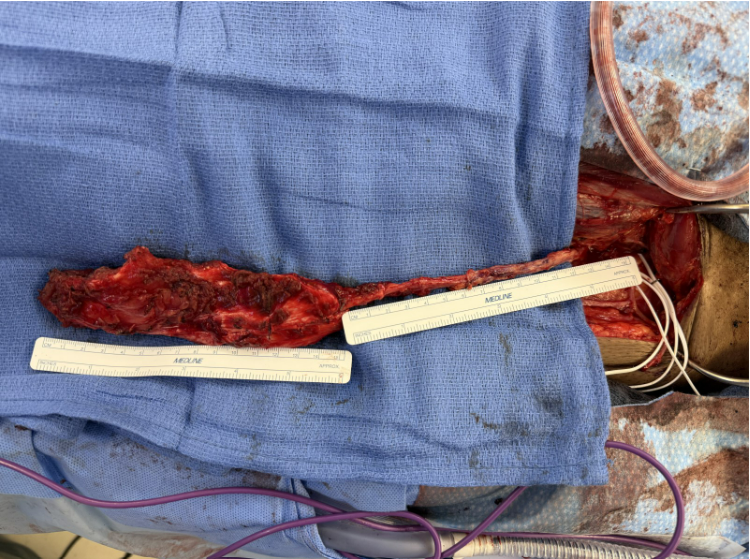
Surgeon’s view of anterolateral thigh flap (muscle-only) that was harvested for reconstruction of the patient’s cranial base defect after endoscopic resection and debridement of the infected bone from the skull base. Source: NYU Langone Health.





