Subtleties Drive Treatment
A series of three cases at NYU Langone Health illustrate how management is evolving for small renal masses (SRMs), says urologic oncologist William C. Huang, MD, a member of the American Society of Clinical Oncology Guidelines Panel for SRMs.
Instead of radical nephrectomy, Dr. Huang and colleagues increasingly opt for kidney-sparing options including active surveillance, ablation, or partial nephrectomy. The shift reflects earlier SRM detection due to imaging advances, plus a relatively low risk of disease progression.
Here, the first two cases were treated with robotic partial nephrectomy, the third, active surveillance.
Dr. Huang notes that currently, the majority of patients with SRMs in the United States still receive immediate, active treatment. He attributes this to reactivity and biases in risk perception.
“Up to 20 percent of surgically resected SRMs are benign. In spite of the exceedingly low risk of cancer spread, there is still a great amount of anxiety among patients and referring providers prompting immediate treatment for cancers that can be appropriately closely monitored.”
“We must educate patients and providers about the very low oncologic risk attributable to SRMs.”
William C. Huang, MD
Oncocytomas, such as in the first case, have overlapping features with malignant renal masses and can appear similar to clear cell renal carcinoma on imaging, Dr. Huang says, emphasizing pretreatment imaging or biopsy to differentiate this benign lesion from kidney cancer. Comprehensive imaging, such as in the second case, can support Bosniak classification but still can fail in accurately differentiating a cystic renal cell carcinoma from a benign complex cyst.
The third case reinforces the need to consider whether a patient will truly benefit from any treatment, regardless of risk. Dr. Huang’s team opted for active surveillance for this patient—who died five months later due to a comorbidity. Says Dr. Huang, “We must educate patients and providers about the very low oncologic risk attributable to SRMs, allowing them to make informed treatment selections.”
Malignant Appearing Small Mass to Oncocytoma
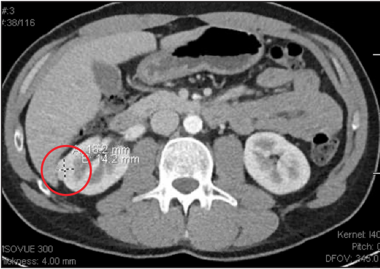
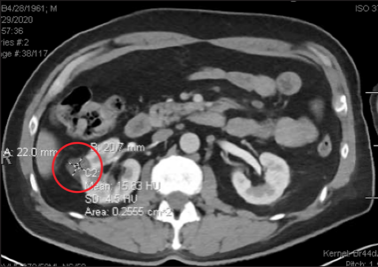
For the first case, a healthy, 39-year-old man presented with abdominal pain, and a CT scan revealed a 2.2 centimeter enhancing solid mass (red circle). The man received a robotic partial nephrectomy. Upon pathology, the excised oncocytoma showed diffuse reactivity for the oncogenic marker CD117 and scattered positivity for CK7. PHOTO: NYU Langone Staff
Benign Multi-Locular Cyst Appears as a Suspicious Malignant Cyst
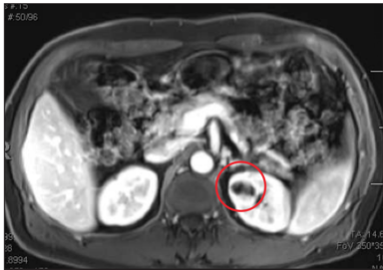
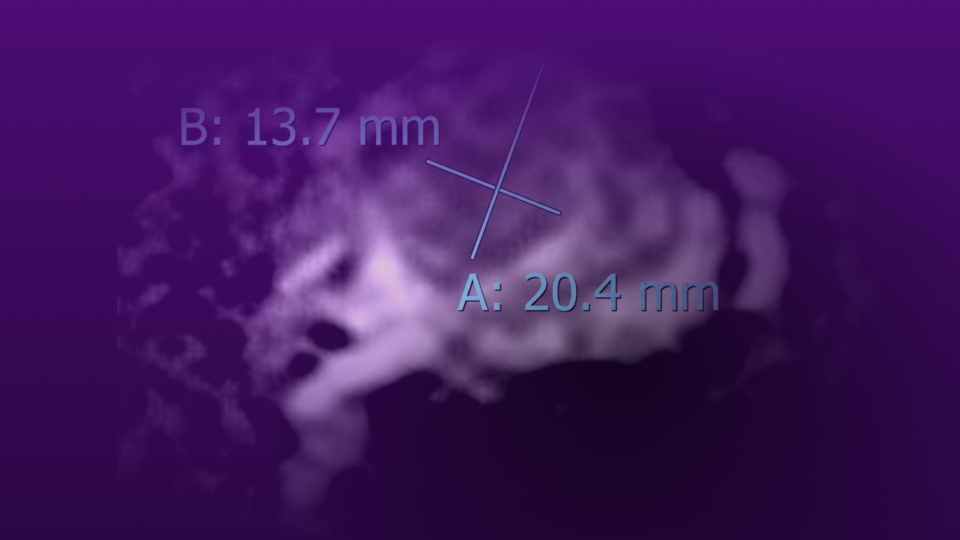
In a second case, providers identified a mass in a healthy 54-year-old man: an incidental 2.5 centimeter complex cyst on chest CT (red circle) that was later confirmed via MRI as a 2.6 centimeter cystic left upper pole renal lesion. The septated mass had a thick rim and was rated Bosniak category III. PHOTO: NYU Langone Staff
Comorbidity Considerations Essential
The third case involved a 59-year-old man with a history of cardiovascular conditions, including coronary artery disease, severe aortic regurgitation, a cerebrovascular accident, and a thoracic aortic aneurysm repair. He had a biopsy-proven, enlarging solid 2.2 centimeter papillary renal cell carcinoma (red circle). PHOTO: NYU Langone Staff