Hip subluxation is common in children with spastic cerebral palsy, and the risk of significant subluxation increases with GMFCS (Gross Motor Function Classification System) level. Patients who are nonambulatory have a much higher risk of subluxation, approaching 90 percent over their lifetime.
Hip screening protocols have been instrumental in recognizing hip subluxation more quickly and accurately. Hip reconstruction, including varus derotational osteotomy (VDRO) with potential addition of pelvic osteotomy, is recommended when hip subluxation exceeds 50 percent. Bilateral hip reconstruction is considered in children with bilateral leg involvement and asymmetric hip subluxation to prevent further subluxation of the less involved hip, maintain pelvic balance, and minimize leg length discrepancy.
Here, we present a case involving a 10-year-old male with spastic quadriplegic cerebral palsy (GMFCS level V) with progressive hip pain, asymmetric subluxation, and increasing leg length discrepancy. The patient underwent bilateral adductor longus tenotomy, proximal femur VDRO, and bilateral pelvic osteotomy (Dega-type). At five years post-surgery, he had maintenance of hip reduction, improved sitting balance, and improved comfort with motion.
The case demonstrates that bilateral hip reconstruction addressing both femur and pelvis in nonambulatory children with spastic cerebral palsy is safe, yields long-lasting results, and can improve comfort and sitting balance.
Case Highlights:
- The patient presented with 75 percent subluxation of the right hip, 35 percent subluxation of the left hip, and a 1.5-cm leg length discrepancy.
- Bilateral pelvic osteotomies were added after intraoperative instability persisted following femoral correction alone.
- At five-year follow-up, the patient maintained stable hip reduction and equal leg lengths, with improved sitting balance, greater comfort with motion, pain-free hips, and continued daily stander use.
Case Presentation
History. The patient is a 10-year-old male with a history of spastic quadriplegic cerebral palsy, GMFCS level V (nonambulatory), who presented for initial evaluation of his hips. He is a former 24-week preemie with history of seizure disorder and mixed tone (spasticity and dystonia). He had extensive and well-coordinated spasticity management with a neurologist and a physiatrist and is on baclofen (both oral and through baclofen pump). BOTOX® (onabotulinumtoxinA) injections had also been tried in the past, but the patient’s parent felt they were ineffective. The parent noted increasing pain in both hips, more pronounced in the right than the left, with diapering, positioning, and physical therapy. The parent also noticed an increasing leg length discrepancy that made use of his stander and sitting for long periods uncomfortable.
Physical Examination. The patient was below the 1st percentile for height and weight. He has pelvic obliquity and a mild scoliosis which is flexible in his thoracolumbar spine. On lower extremity exam, he holds his right hip adducted with abduction only to neutral before activation of dystonia. Left hip abducts 20 degrees. Significant discomfort with rotation of both hips, particularly the right. Hip flexion limited to 80 degrees bilaterally, internal rotation to 80 degrees, external rotation to 30 degrees. Popliteal angles are greater than 60 degrees bilaterally without significant knee flexion contracture. He has a leg length discrepancy of 1.5 cm with right side being shorter. He has both spasticity and dystonia on exam. Dystonia is more marked in his upper extremities and neck. Radiographs of the pelvis showed a 75 percent subluxation of the right with 35 percent subluxation on the left as well as pelvic obliquity (Figure 1). Preoperative neck-shaft angles measured about 145 degrees.

Preoperative Optimization. The patient was evaluated in our complex pediatric preoperative clinic. Nutrition was optimized preoperatively (BMI increased from 13 to 15.5), and baclofen pump dosage was increased in preparation for surgery. Preoperative pulmonary evaluation and sleep study was also performed.
Surgical Procedure
The patient underwent bilateral fascia iliaca blocks in addition to general anesthesia. Tranexamic acid (TXA) was used to minimize blood loss during the procedure. Patient underwent bilateral adductor longus tenotomy to increase abduction, proximal femur VDRO, and pelvic osteotomy. A bilateral procedure was chosen to prevent further left hip subluxation and minimize leg length discrepancy, which was causing difficulty using his stander. A 90 degree cannulated blade plate was chosen to allow for correction of his neck-shaft angle and anteversion. A 1-cm wedge on the right and a 2-cm wedge of the left was removed at the level of the lesser trochanter in order to facilitate correction and equalization of leg lengths.
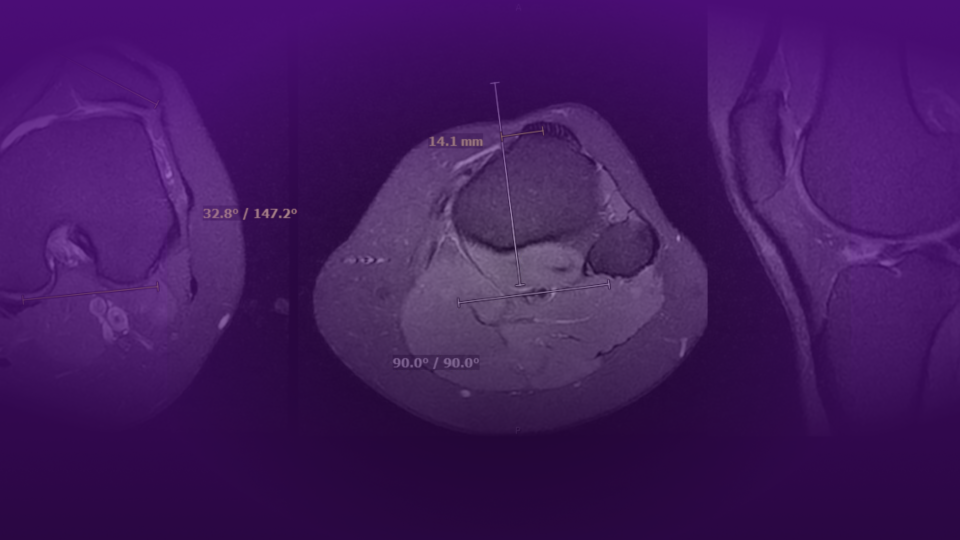
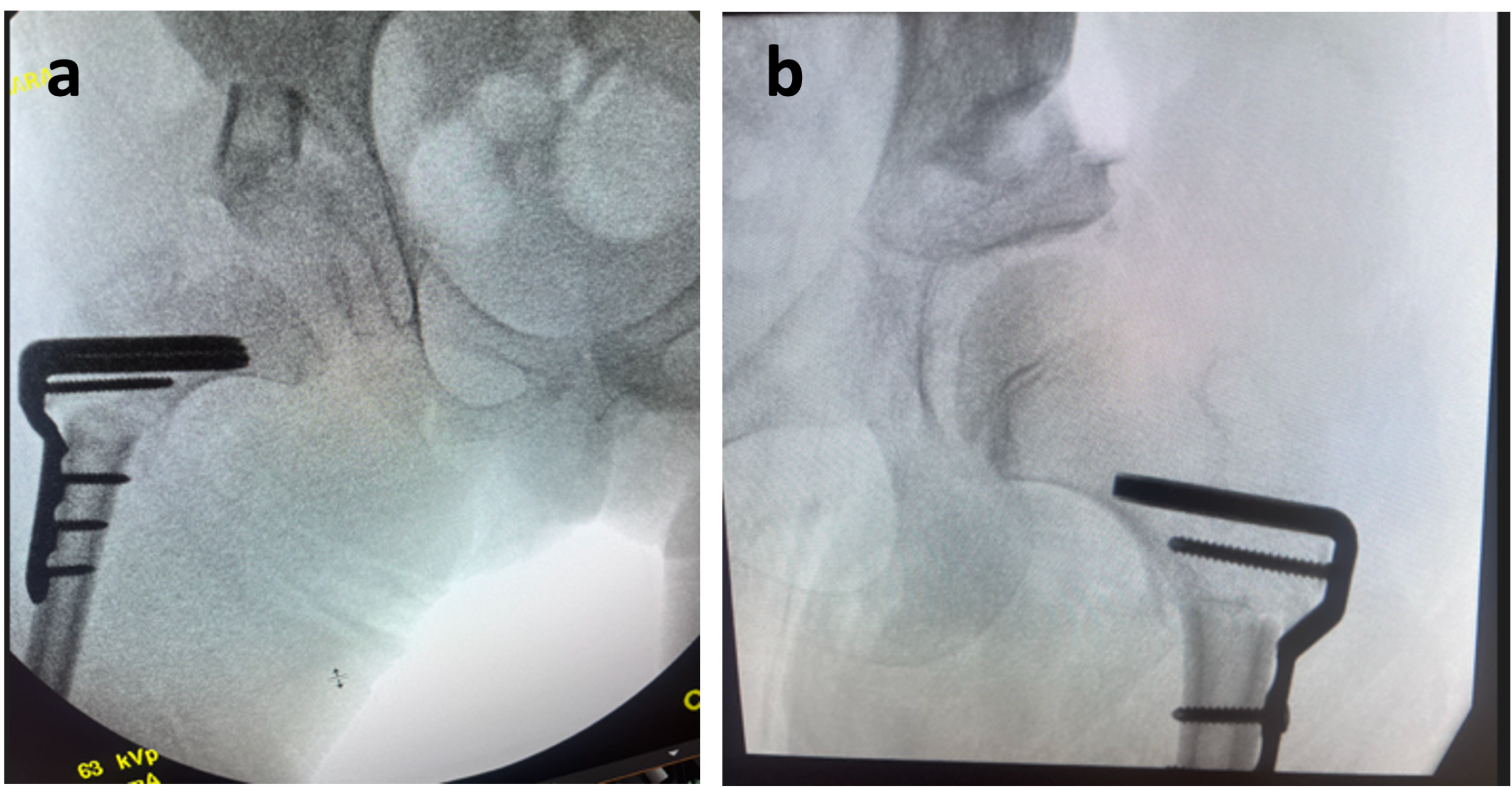
The decision for pelvic osteotomy was made intraoperatively after VDRO and based on fluoroscopic stability exam in common positions of subluxation/dislocation. Both hips subluxated in greater than neutral adduction and flexion/internal rotation. Of note, his acetabular index on the left as well as migration percentage had increased significantly from preoperative radiographs during the five months it took for medical optimization. A Dega-type osteotomy was performed bilaterally with an osteotome in order to increase posterior coverage. A laminar spreader was used to gently lever open the osteotomy site, and the wedges of bone removed from his femur were inserted (Figure 2). Abduction pillow used for postoperative comfort and immobilization. Patient was discharged to home on POD2. He was allowed to be weight-bearing as tolerated.
Follow-Up
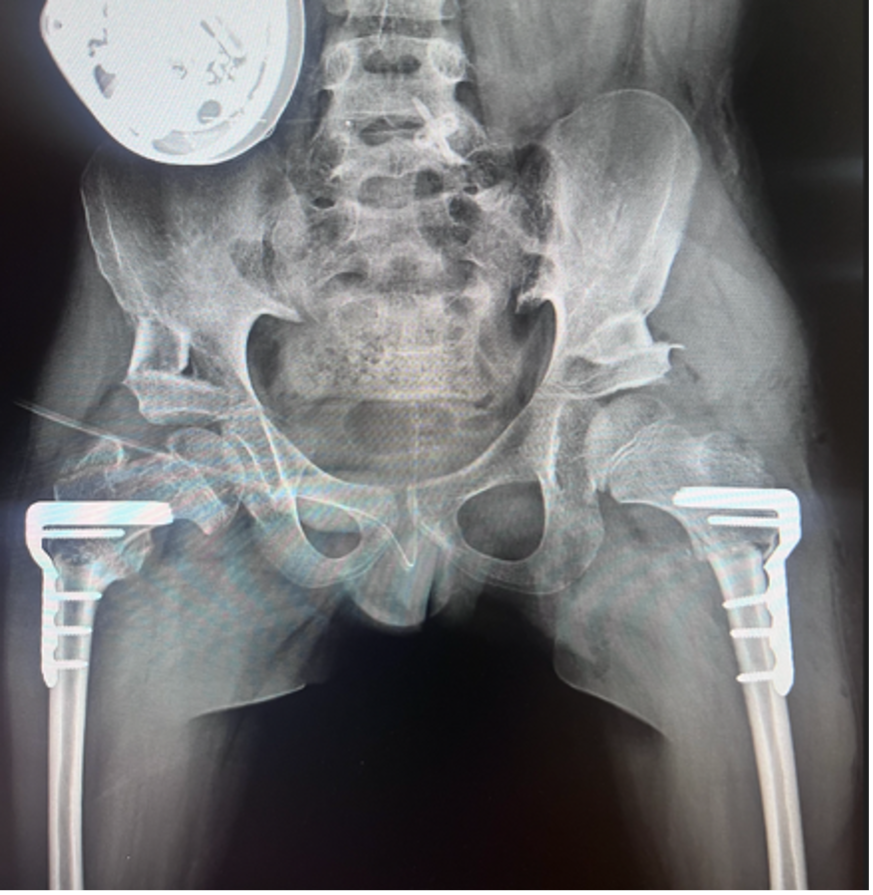
Home physical therapy was initiated the week after discharge. Subsequent imaging at six weeks postoperatively showed healing at the femoral osteotomy sites and significant improvement in pelvic obliquity (Figure 3). He returned to school and his physical and occupational therapy regimen, including use of his stander.
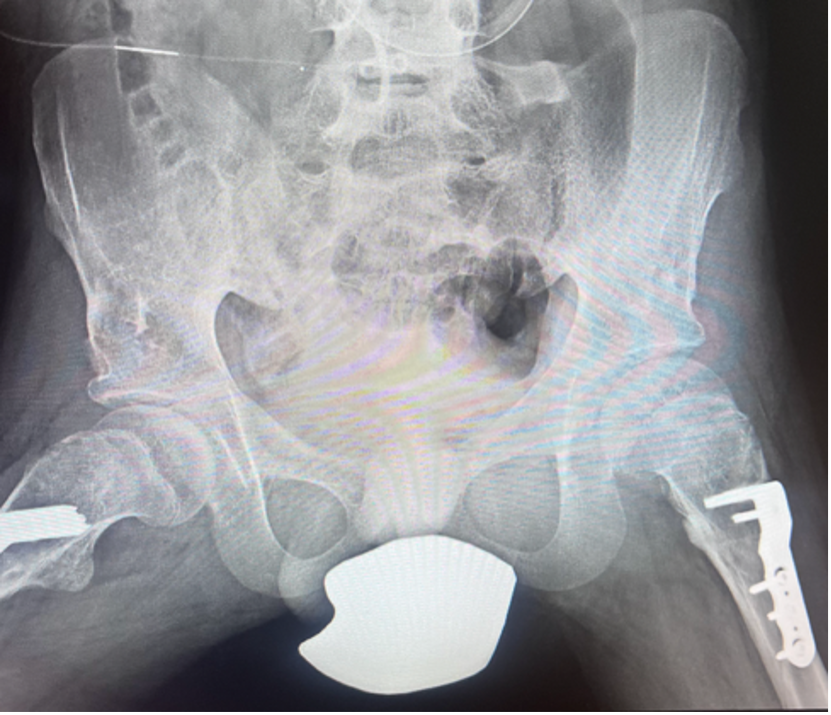
His most recent follow up radiographs at five years postoperatively show continued appropriate coverage of bilateral hips, which are now more mobile and pain free (Figure 4). He now uses his stander for one hour a day, and he has maintained equal leg lengths. He continues to sit well in his wheelchair. His family has elected not to remove femoral plates, which is often offered at one year after initial reconstruction. Family did elect to remove his baclofen pump and transition to oral medication for tone management.
Conclusion
Bilateral hip reconstruction in children with spastic cerebral palsy, addressing both proximal femur and pelvic pathology when needed, yields long-lasting maintenance of hip reduction and promotion of improved pelvic balance while minimizing leg length inequality.