Muscle-invasive bladder cancer (MIBC) with variant histology, particularly small cell/neuroendocrine differentiation, is traditionally associated with aggressive clinical behavior and a high risk of early dissemination. As such, management has historically favored aggressive approaches, including chemotherapy and radical extirpation in many cases.
However, evolving systemic therapy regimens and improved multidisciplinary coordination are increasingly allowing for individualized and potentially bladder-preserving treatment pathways in carefully selected patients.
At NYU Langone Health, we emphasize a patient-centered, multidisciplinary approach that integrates systemic therapy response, pathologic findings, and functional goals when determining definitive management. Illustrating this approach, this Case of the Month highlights a patient in his early 80s with variant MIBC whose excellent response to chemotherapy enabled bladder-preserving consolidation rather than immediate radical cystectomy.
Case Highlights:
- The patient presented with MIBC with small cell, sarcomatoid, and squamous variant histology of urothelial cell carcinoma.
- Given concern for locally advanced disease and nodal involvement, he was treated with cisplatin and etoposide-based systemic chemotherapy, achieving a marked response.
- Following multidisciplinary reassessment supporting bladder-sparing consolidation, he underwent robotic-assisted partial cystectomy with pelvic lymph node dissection.
- Final pathology confirmed ypT0N0 status (no residual carcinoma), and he experienced excellent postoperative recovery with preserved bladder function.
Case Presentation
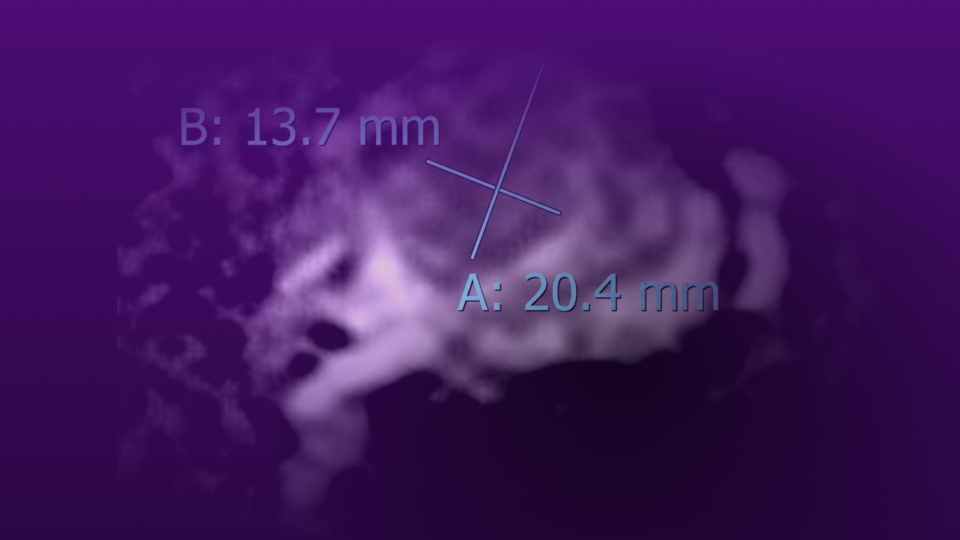
A man in his early 80s presented with MIBC characterized by variant histology, including small cell, sarcomatoid, and squamous differentiation. Initial staging raised concern for locally advanced disease with associated lymphadenopathy.
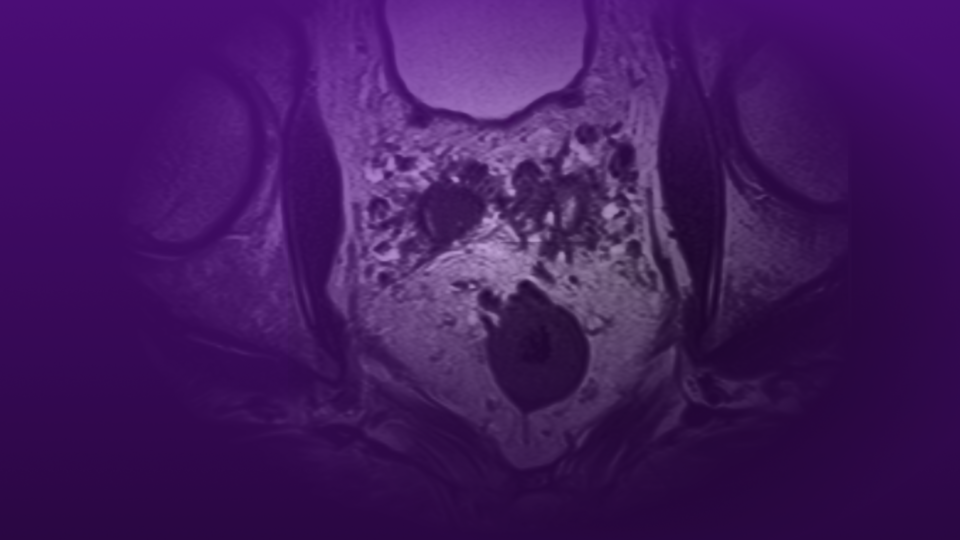
Given the aggressive histologic features, the patient was treated with cisplatin and etoposide-based systemic chemotherapy. He tolerated therapy well and demonstrated a significant clinical response, with marked improvement in bladder tumor burden and resolution of previously concerning radiographic findings.
Following completion of systemic therapy, the patient was re-evaluated in a multidisciplinary setting. Given his excellent response, absence of definitive metastatic disease, and strong functional status, he was felt to be an appropriate candidate for bladder-preserving consolidation rather than immediate radical cystectomy.
Surgical Management and Outcome
The patient underwent robotic-assisted partial cystectomy with pelvic lymph node dissection.
His postoperative course was uncomplicated. The Foley catheter was removed, and he successfully resumed clean intermittent catheterization (CIC) without difficulty. He reported no hematuria, maintained normal bowel function, and returned to independent ambulation and normal diet.
At follow-up, he was performing CIC twice daily with low residual volumes of approximately 100 to 200 mL and reported a meaningful improvement in urinary comfort and overall quality of life. Plans were established for the patient to discontinue self catheterization early.
- Final pathology demonstrated an excellent oncologic response, including:
- Bladder specimen: no residual carcinoma, only focal urothelial atypia
- Pelvic lymph nodes (right and left): all negative for cancer
- Diverticulum specimen: benign urothelial changes with focal mild atypia
- Overall staging: ypT0N0
Discussion
This case highlights the evolving role of multimodal bladder-preserving strategies in selected patients with variant histology muscle-invasive bladder cancer.
While small cell bladder cancer is typically associated with aggressive behavior, it is also among the most chemotherapy-sensitive subtypes of urothelial carcinoma. In this case, treatment with cisplatin and etoposide resulted in a profound response, allowing for reconsideration of definitive surgical strategy.
At NYU Langone Health, multidisciplinary collaboration between urologic oncology, medical oncology, radiation oncology, and pathology is central to individualized decision-making. This approach enables careful reassessment of disease biology after systemic therapy and supports bladder preservation in appropriately selected patients.
The final pathology demonstrating ypT0N0 disease following partial cystectomy underscores both the chemosensitivity of this tumor subtype and the importance of reassessing treatment pathways in responders.
Equally important, the patient achieved an excellent functional outcome, maintaining bladder function with a minimally invasive surgical approach and returning to a high quality of life postoperatively.
Conclusion
This case demonstrates that even in the setting of high-risk variant histology MIBC, durable oncologic control and bladder preservation may be achievable in carefully selected patients who demonstrate a robust response to systemic chemotherapy.
Through a coordinated multidisciplinary approach, NYU Langone Urology continues to expand treatment possibilities for complex bladder cancer patients—balancing oncologic rigor with preservation of function and quality of life.