Testicular cancer represents the most common solid malignancy in men aged 15 to 40, with approximately 10,000 new cases diagnosed each year, and cure rates exceed 95 percent across all stages. As such, long-term survivorship—including preservation of reproductive function—should be a central consideration in treatment planning.1,2,3,4
Yet, despite the critical importance of fertility preservation, contemporary data reveal that oncofertility counseling and sperm cryopreservation remain significantly underutilized. Studies report that only 10 to 50 percent of eligible men with newly diagnosed cancer undergo sperm banking prior to treatment, even though both the American Society of Clinical Oncology (ASCO) and the American Urological Association (AUA) recommend that fertility preservation be discussed with all patients of reproductive age prior to gonadotoxic therapy.5,6,7
Here, we present three cases that highlight the range of fertility-related challenges faced by young men with urologic malignancies. These cases underscore the important role urologists play in incorporating oncofertility into cancer care from the outset—not as a secondary consideration, but as a routine part of the initial treatment discussion.
Case Highlights:
- The first two cases involve successful conception following treatment.
- The third case involves bilateral disease managed with testis-sparing surgery; the patient underwent pretreatment sperm cryopreservation, with postoperative semen analysis also demonstrating viable sperm.
- Sperm banking can typically be completed within 24 to 72 hours and rarely delays treatment, with TESE and other techniques available for pre-existing azoospermia.
- Semen analysis should be incorporated into survivorship care, as spermatogenesis recovery may continue for years after treatment completion.
Case Presentation 1
A newly married man in his late 20s presented for fertility workup. Semen analysis ordered by his primary care physician showed oligospermia (8 million sperm/mL). Physical exam revealed a painless left testicular mass and ultrasound revealed a 3.1 cm solid hypoechoic intratesticular lesion with increased vascularity. Serum tumor markers showed an elevated alfa-fetoprotein (AFP) (85 ng/mL) and normal beta human chorionic gonadotropin (β-hCG) and lactate dehydrogenase (LDH). He and his wife had been actively trying to conceive.
Management. The patient underwent pretreatment sperm cryopreservation (two specimens banked) followed by left radical inguinal orchiectomy. Staging CT and post-orchiectomy markers were consistent with clinical stage IA nonseminomatous germ cell tumor. The patient was placed on active surveillance.
Fertility Outcome. At 12 months post-orchiectomy, repeat semen analysis demonstrated persistent oligospermia. The patient and his wife conceived successfully via intrauterine insemination using cryopreserved sperm at 18 months post-treatment.
Case Presentation 2
A man in his early 30s with no significant past medical history was diagnosed with a 7 cm testicular mass, found to be clinical stage IIA pure seminoma (cT1N1M0S1). He was unmarried at the time and had no children but expressed a strong desire for future fertility. Pre-treatment semen analysis was normal. He was counseled regarding the gonadotoxic effects of chemotherapy.
Management. The patient underwent pretreatment sperm cryopreservation (three specimens banked) followed by three cycles of BEP (bleomycin, etoposide, cisplatin). Post-chemotherapy imaging demonstrated a complete radiographic response.
Fertility Outcome. At six months post-chemotherapy, semen analysis revealed azoospermia. By 18 months, spermatogenesis partially recovered (4 million sperm/mL). At 24 months, the patient achieved natural conception with his partner without use of banked sperm.
Case Presentation 3
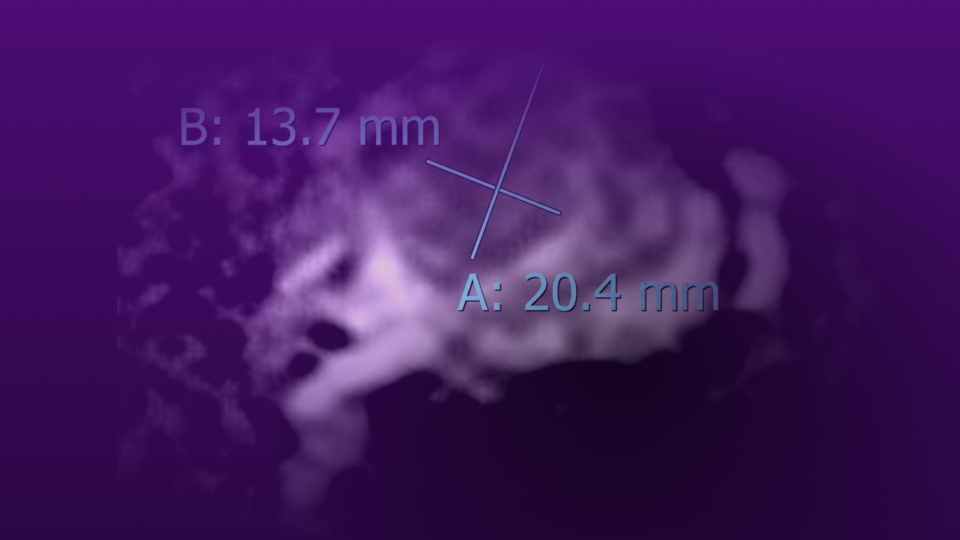
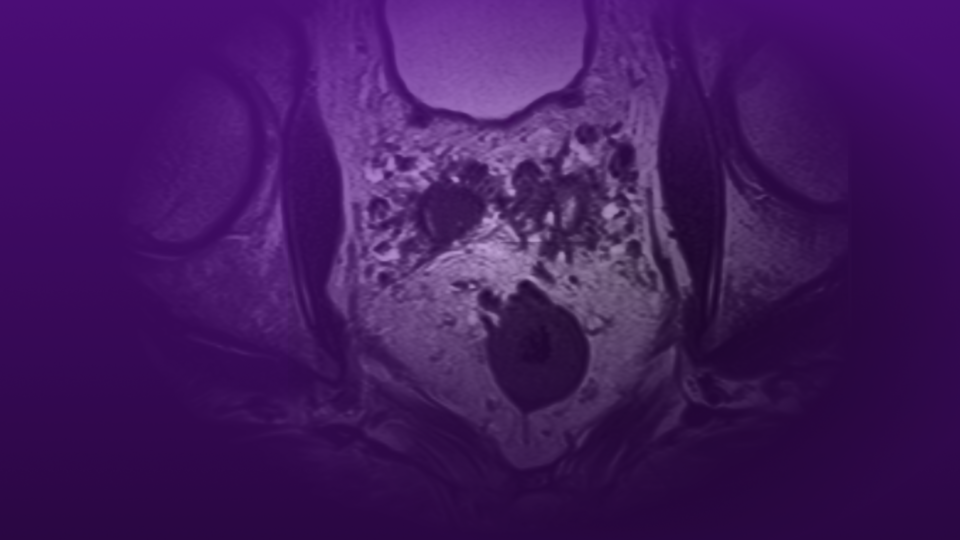
A man in his mid 30s with a history of right orchiectomy for seminoma (stage IA, on surveillance) five years prior presented with a new 1.8 cm hypoechoic lesion in the remaining left testicle on routine surveillance ultrasound. Tumor markers were normal. He has two children and had not previously banked sperm. He was counseled extensively regarding the implications of a second orchiectomy, including permanent hypogonadism and infertility.
Management. He underwent urgent sperm cryopreservation followed by partial orchiectomy (testis-sparing surgery), with intraoperative frozen section confirming negative margins.
Fertility Outcome. Post-operative testosterone levels remained in the low-normal range (285 ng/dL), and the patient did not require testosterone replacement. Semen analysis at six months showed severe oligospermia (1.5 million sperm/mL) but viable sperm, preserving the option for assisted reproduction.
Discussion
The Impact of Disease and Treatment on Fertility. Testicular cancer itself impairs spermatogenesis. At the time of diagnosis—before any treatment—up to 50 to 60 percent of testicular cancer patients demonstrate abnormal semen parameters, including oligospermia or azoospermia. The etiology is multifactorial and includes testicular dysgenesis, contralateral testicular dysfunction, and the systemic effects of malignancy.8,9
Treatment further compounds this risk. While unilateral orchiectomy alone has a relatively modest impact on long-term fertility in men with a normal contralateral testis, the addition of chemotherapy—particularly cisplatin-based regimens—poses a dose-dependent risk of prolonged or permanent azoospermia. Retroperitoneal lymph node dissection (RPLND), when performed, carries a risk of retrograde ejaculation due to disruption of sympathetic nerve fibers, though nerve-sparing techniques have reduced this complication to fewer than 5 percent of cases at experienced centers. Radiation therapy to the para-aortic field, used in select seminoma cases, can scatter to the remaining testis and transiently suppress spermatogenesis.1,10
Recovery of spermatogenesis after chemotherapy is time- and dose-dependent. Following BEP chemotherapy, approximately 80 percent of men recover sperm production within two to five years, though cumulative cisplatin dose is the strongest predictor of prolonged impairment. Patients receiving four or more cycles face a substantially higher risk of persistent azoospermia compared to those receiving one to two cycles.8,11,12
Barriers to Fertility Preservation. Despite guideline recommendations, multiple barriers contribute to the underutilization of sperm cryopreservation:
- Urgency of treatment initiation: Providers and patients may perceive a time pressure to begin cancer-directed therapy, though sperm banking typically requires only 24 to 72 hours and rarely delays treatment.
- Inadequate counseling: Studies consistently demonstrate that a significant proportion of oncology patients do not recall receiving fertility counseling, suggesting either that discussions are not occurring or are insufficiently emphasized.
- Cost and access: Sperm cryopreservation costs approximately $500 to $1,500 for initial banking, with annual storage fees of $200 to $500, and insurance coverage remains inconsistent. Geographic access to reproductive medicine services is also limited in many regions.
- Baseline impairment: Patients with pre-existing azoospermia may be told that banking is not possible, though advanced techniques such as testicular sperm extraction (TESE) can retrieve viable sperm in some of these men.
Special Considerations: Bilateral Disease and Testis-Sparing Surgery. As illustrated in Case 3, metachronous bilateral testicular tumors occur in 2 to 5 percent of testicular cancer survivors. In this setting, testis-sparing surgery (partial orchiectomy) has emerged as a viable strategy to preserve both hormonal function and fertility potential, provided the tumor is amenable to complete excision with negative margins. European guidelines support this approach for tumors less than 2 cm in a solitary testis, with adjuvant local radiation considered to address the risk of associated germ cell neoplasia in situ (GCNIS)—though radiation to the remaining testicular parenchyma will likely render the patient infertile, underscoring the importance of pre-operative sperm banking.13,14,15,16
A Call to Action
These cases illustrate the spectrum of fertility challenges facing young men with urologic malignancies, and many of these ideas can be translated to non-urologic malignancies as well. As urologists, we are uniquely positioned to integrate oncofertility into the treatment paradigm—not as an afterthought, but as a standard component of the initial consultation.
Key principles include:
- Universal counseling: All men of reproductive age should receive fertility counseling at the time of cancer diagnosis, regardless of current parental status or stated reproductive goals.
- Pre-treatment cryopreservation: Sperm banking should be offered before orchiectomy when feasible, as semen quality may decline further after surgery.
- Multidisciplinary collaboration: Early referral to reproductive medicine specialists ensures that patients have access to the full range of fertility preservation options, including TESE for azoospermic patients.
- Longitudinal follow-up: Semen analysis should be incorporated into survivorship care, as spermatogenesis recovery may continue for years after treatment completion.
References
- Singla N, et al. JAMA.2025;333(9):793–803. DOI.
- Miller KD, et al. CA Cancer J Clin. 2020;70(6):443-459. DOI.
- Cheng L, et al. Nat Rev Dis Primers. 2018;4(1):29. DOI.
- Baird DC, et al. Am Fam Physician. 2018;97(4):261-268. Link.
- Schlegel PN, et al. J Urol. 2021;205(1):44-51. DOI.
- Su HI, et al. J Clin Oncol. 2025;43(12):1488-1515. DOI.
- Alexander MV, et al. Oncologist. 2025;30(12):oyaf280. DOI.
- Feldman DR, et al. JAMA. 2008;299(6):672-684. DOI.
- Badia RR, et al. Urol Oncol. 2023;41(3):151.e11-151.e15. DOI.
- Heidenreich J, Heidenreich A. J Clin Oncol. 2025;43(Suppl 5):641. DOI.
- Bujan L, et al. Fertil Steril. 2013;100(3):673-680. DOI.
- Lampe H, et al. J Clin Oncol. 1997;15(1):239-245. DOI.
- Bojanic N, et al. J Surg Oncol. 2015;111(2):226-230. DOI.
- Maroto P, et al. Urol Oncol. 2021;39(2):135.e17-135.e23. DOI.
- Testicular Cancer. NCCN. Updated 2025-10-15. Link.
- Heidenreich A, et al. J Urol. 2001;166(6):2161-2165. DOI.