

Three Failing Organs and a Rare Autoimmune Disease
Almost 15 years ago, a then-26-year-old man with a history of Goodpasture syndrome received a kidney transplant from his brother. In 2021, he presented to an emergency room in Brooklyn with symptoms of severe heart failure. After his symptoms progressed, he was referred to cardiologist Bernard S. Kadosh, MD, an assistant professor of medicine at NYU Langone Health’s Heart Failure Advanced Care Center, who found evidence of restrictive cardiomyopathy—highly unusual for someone his age.
After an initial echocardiogram and PYP scan, Dr. Kadosh established a working diagnosis of cardiac amyloidosis; however, given the patient’s age, he was sent for confirmatory genetic testing, which ruled out hereditary amyloidosis. A follow-up endomyocardial biopsy was also conducted and was consistent with this finding.
“We didn’t know exactly what was wrong, but we knew what the treatment was—he needed a heart transplant,” Dr. Kadosh says.
“We didn’t know exactly what was wrong, but we knew what the treatment was—he needed a heart transplant.”
Bernard S. Kadosh, MD
As the patient’s condition continued to deteriorate, further tests revealed that he would also need a lung and kidney transpant.
“His pulmonary pressures were extremely high and irreversible,” Dr. Kadosh explains. “The kidney that he’d received years earlier was rapidly failing.”
After a multidisciplinary discussion, specialists from the NYU Langone Transplant Institute decided the patient needed a triple organ transplant: heart, lungs, and kidney. He was admitted to the hospital, where he waited for two months until a suitable donor became available.
In March 2022, a team of transplant surgeons including Nader Moazami, MD, Deane E. Smith, MD, Stephanie H. Chang, MD, Jonathan Berger, MD, and clinical specialists conducted a 13-hour operation to successfully transplant the organs he needed, making this the first successful triple transplant for heart, lungs, and kidney in the Northeast.
Three months after surgery, the patient is doing well, with additional diagnostic studies ongoing.
“Due to consistently high calcium levels, our working diagnosis is tertiary hyperparathyroidism as a result of the failed kidney transplant, but we are still waiting for more definitive results,” Dr. Kadosh says.
“Few transplant programs would have the expertise to take on a case like this due to the high degree of technical complexity,” Dr. Kadosh observes. “Our unique skills and experience, combined with our robust clinical infrastructure, gave us certainty that we could be successful.”
An Unexpected Finding: Not Amyloidosis
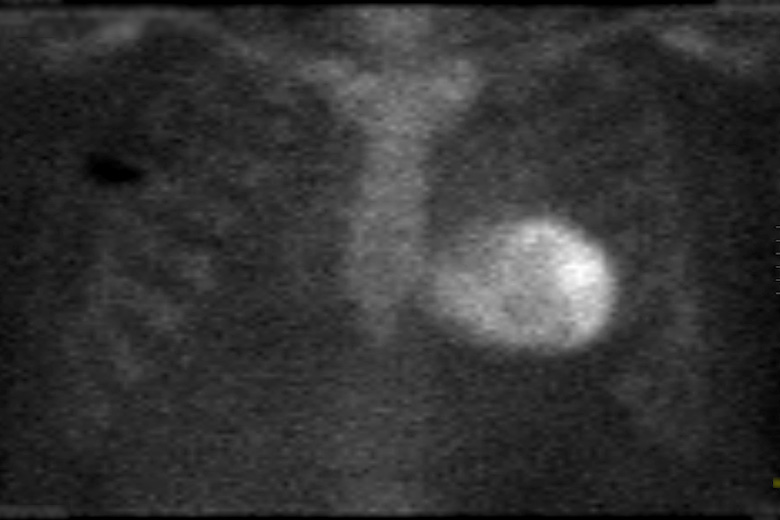
The patient’s Tc-99m PYP scan on admission. SOURCE: NYU Langone Staff
On admission, the patient’s PYP scan was highly positive, the most positive that Dr. Kadosh and team had ever seen, yet genetic testing and endomyocardical biopsy confirmed that the diagnosis was not cardiac amyloidosis.
High Pulmonary Pressures
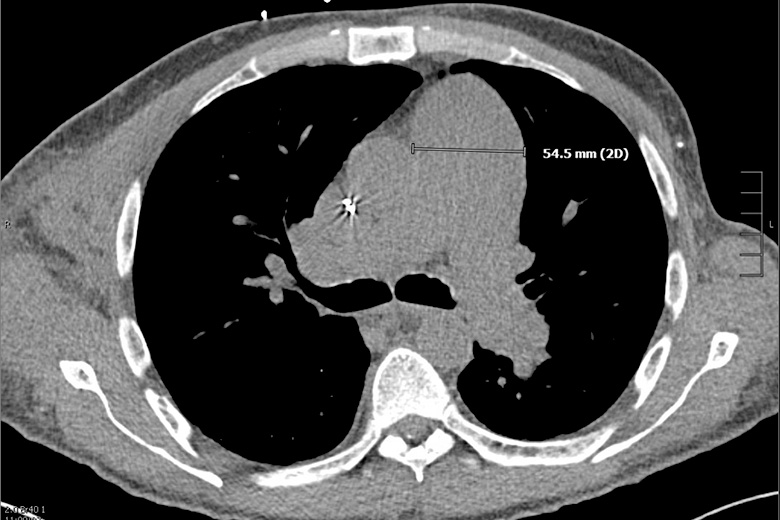
The patient’s CT scan after his initial workup. SOURCE: NYU Langone Staff
A CT scan showed irreversible pulmonary hypertension, indicating that the patient could not undergo a heart and kidney transplant alone—he would not survive the surgery. Other tests revealed the kidney he received almost two decades earlier was rapidly failing.
A Complex Procedure

SOURCE: NYU Langone Staff
The patient was admitted into the hospital, and had to wait two months for a suitable donor. A large team of doctors and nurses from the NYU Langone Transplant Institute conducted a 13-hour operation to successfully transplant the organs.
Massive Calcification
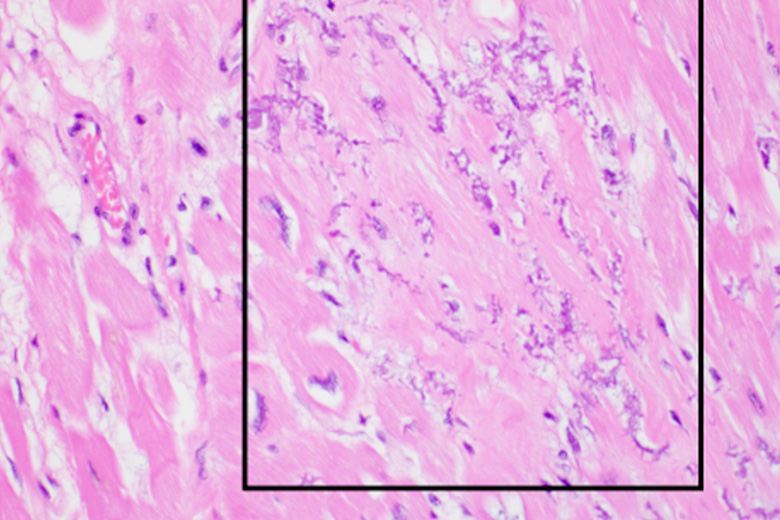
A stained slide showing calcification in myocytes. SOURCE: NYU Langone Staff
Surgical pathology from the cardiac explant revealed extensive microcalcification within the myocyte cytoplasm and cardiac interstitium involving the entire left ventricle and both atria. Further studies showed consistently elevated serum calcium and parathyroid hormone levels, suggesting the cause of his symptoms was tertiary hyperparathyroidism secondary to the failing kidney graft.



